Downloaded 56 times
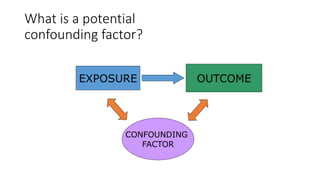
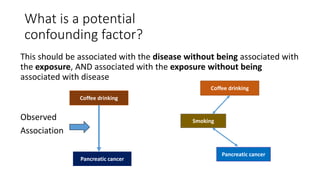

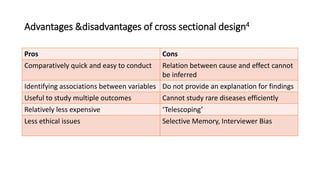
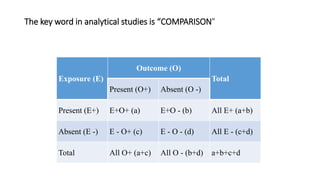
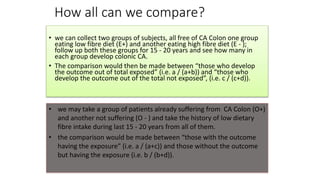
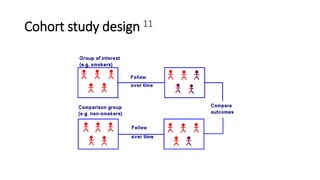
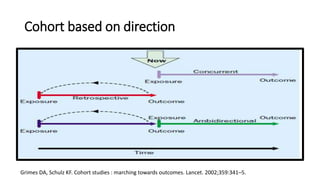
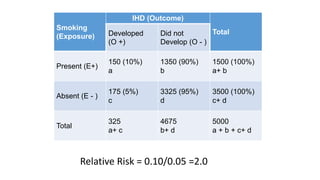
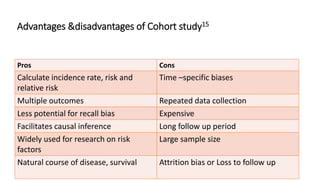
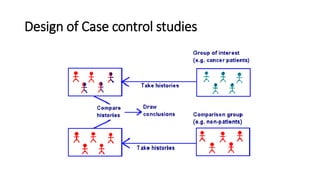
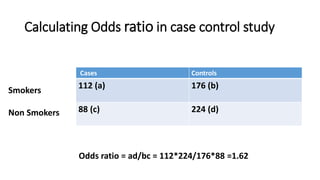
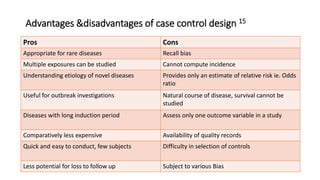
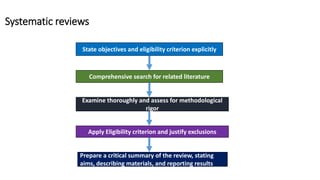
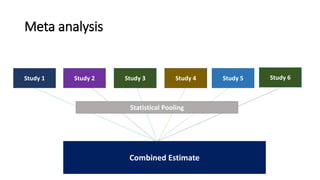


This document discusses various study designs used in epidemiology, including measures of disease occurrence such as prevalence and incidence. It defines prevalence as the total number of cases of a disease at a specified time, while incidence refers to the number of new cases that occur over a period of time. Cohort studies are described as following groups over time to compare rates of an outcome between those exposed and unexposed to a factor. Case-control studies select groups based on having or not having an outcome and look back to compare exposures. Biases such as selection, information and confounding are also outlined.































































