

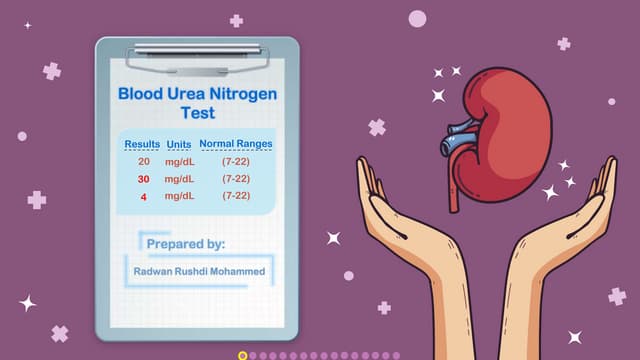
This document discusses various renal function tests and concepts related to glomerular filtration rate (GFR) and tubular handling of substances. It defines GFR and factors affecting it. It also defines related concepts like plasma load, tubular load, transport maximum, and renal threshold. It discusses the importance of plasma clearance and defines osmolar clearance and free water clearance. It also discusses methods of measuring GFR including creatinine clearance (CCR) and estimated GFR (eGFR). It concludes by defining albumin-to-creatinine ratio (ACR) and its significance in evaluating kidney function.



























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



