Downloaded 307 times
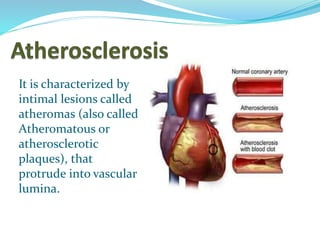
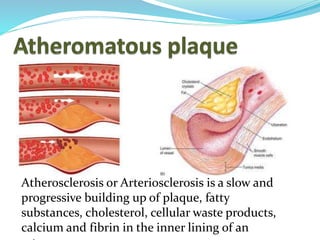

This document provides information about Dr. Tasnim Ara Jhilky, who is an MD in Biochemistry and a phase-A student at Sir Salimullah Medical College. It then discusses atherosclerosis, including its characteristics, pathogenesis, components of atherosclerotic plaques, and prevention methods. It also covers classifications of hyperlipoproteinemia, abnormalities in plasma lipoproteins, and specific types of hyperlipoproteinemia and hypolipoproteinemia.















































































