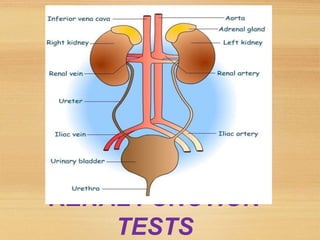
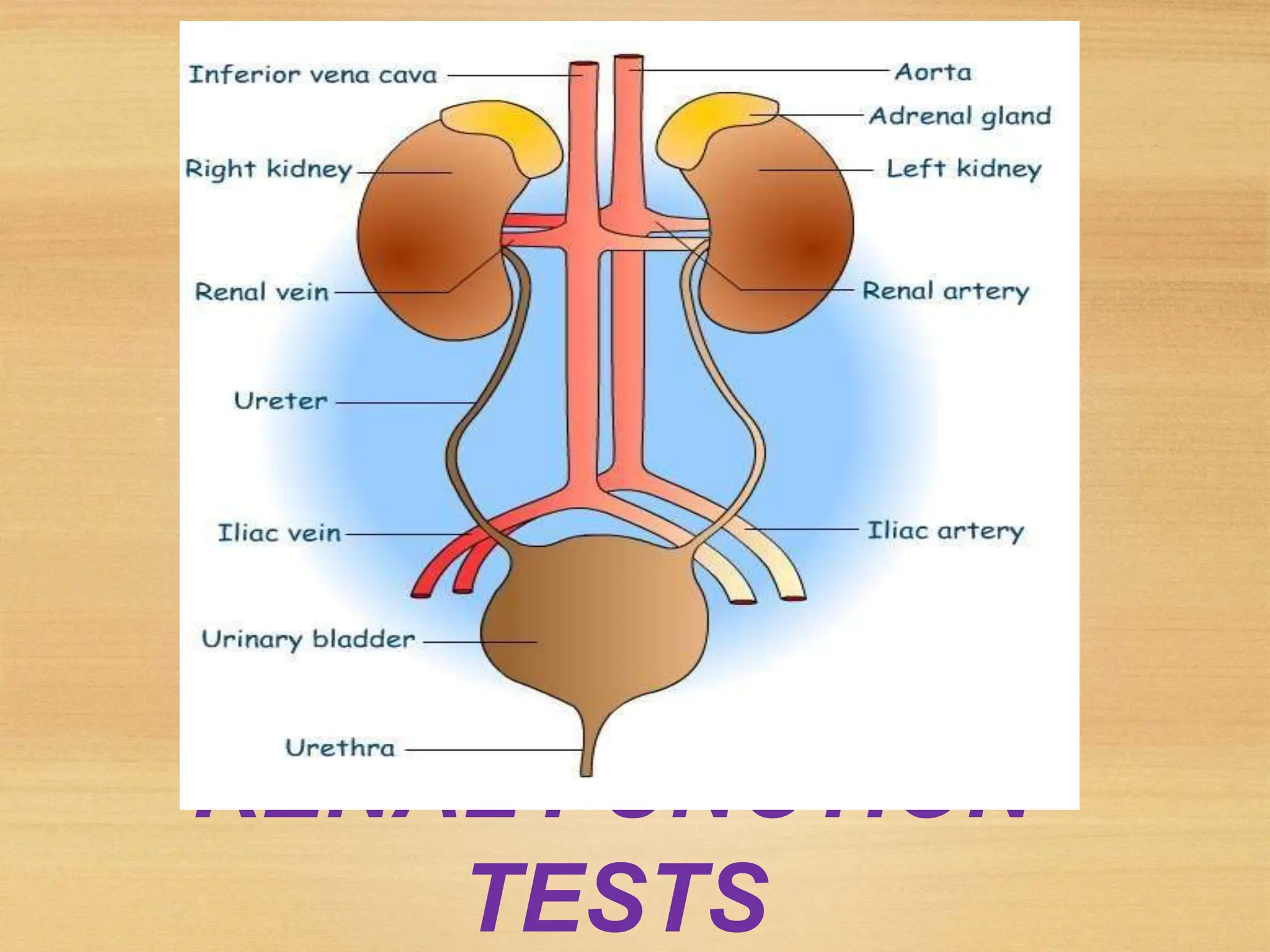
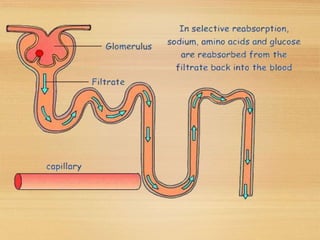
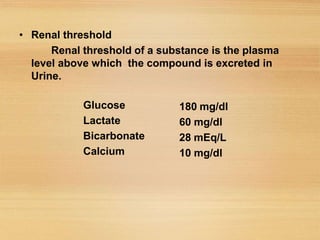
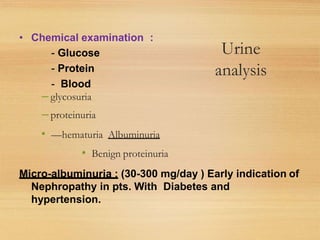
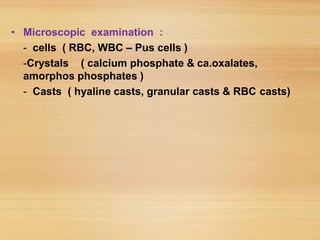
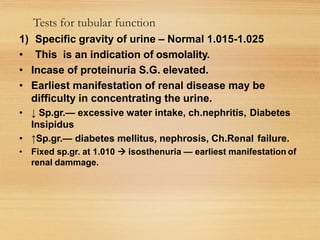
This document discusses renal function tests (RFTs). It begins by describing the functions of the kidney including formation of urine, excretion of waste products, and regulation of water and electrolytes. It then outlines the purposes of RFTs which are to assess renal damage, monitor disease progression, and adjust medication doses. RFTs measure glomerular function through tests of renal clearance and blood analytes like creatinine and urea. They also study tubular function using urine concentration, dilution, and other specialized tests. Common RFTs and their clinical significance are described in detail.