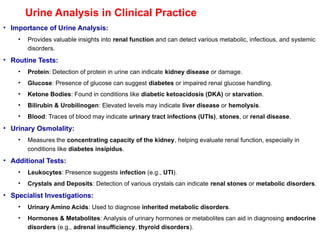
Urine Analysis inClinical Practice
• Importance of Urine Analysis:
• Provides valuable insights into renal function and can detect various metabolic, infectious, and systemic
disorders.
• Routine Tests:
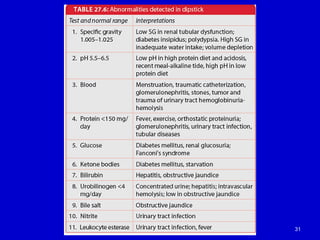
• Protein: Detection of protein in urine can indicate kidney disease or damage.
• Glucose: Presence of glucose can suggest diabetes or impaired renal glucose handling.
• Ketone Bodies: Found in conditions like diabetic ketoacidosis (DKA) or starvation.
• Bilirubin & Urobilinogen: Elevated levels may indicate liver disease or hemolysis.
• Blood: Traces of blood may indicate urinary tract infections (UTIs), stones, or renal disease.
• Urinary Osmolality:
• Measures the concentrating capacity of the kidney, helping evaluate renal function, especially in
conditions like diabetes insipidus.
• Additional Tests:
• Leukocytes: Presence suggests infection (e.g., UTI).
• Crystals and Deposits: Detection of various crystals can indicate renal stones or metabolic disorders.
• Specialist Investigations:
• Urinary Amino Acids: Used to diagnose inherited metabolic disorders.
• Hormones & Metabolites: Analysis of urinary hormones or metabolites can aid in diagnosing endocrine
disorders (e.g., adrenal insufficiency, thyroid disorders).
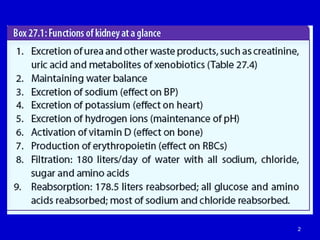
Glomerular Filtration Rate(GFR)
• Definition:
• GFR is the rate at which the kidneys filter blood, specifically how much plasma
is filtered through the glomeruli per minute.
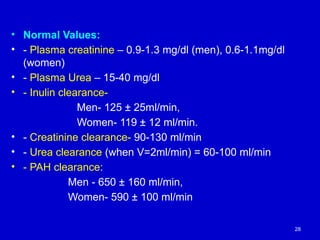
• Normal Values:
• Normal GFR: 120–125 mL/min for a person with a body weight of 70 kg.
• Glomerular filtrate formed: 170-180 liters/day.
• Urine excreted: Only 1.5 liters/day of filtrate is excreted as urine.
• Factors Affecting GFR:
• Blood Pressure: GFR decreases if blood pressure falls below 80 mmHg.
• Renal Obstruction: GFR is reduced when there is obstruction to renal blood
flow (e.g., kidney stones, enlarged prostate).
• Age: GFR naturally declines with aging.
• Renal Blood Flow:
• The renal blood flow is about 700 mL of plasma or 1200 mL of blood per
minute.
6.
Tubular Function inthe Kidney
• Role of Renal Tubules:
• Renal tubules make up 95% of the renal mass and are responsible for modifying the
ultrafiltrate into urine.
• They perform the bulk of the metabolic work in the kidney.
• Key Functions of the Renal Tubules:
• Acid-Base Balance: Regulation of hydrogen ion secretion and bicarbonate
reabsorption.
• Sodium Excretion: Control of sodium retention or excretion based on the body's needs.
• Urine Concentration/Dilution: Adjusting the concentration of urine to maintain water
balance.
• Water Balance: Regulating water reabsorption to maintain body hydration.
• Potassium Excretion: Control of potassium levels in the body through secretion into the
urine.
• Small Molecule Metabolism: Such as inulin clearance and other metabolic functions.
• Clinical Relevance:
• Measuring tubular function directly is impractical for daily clinical use, but it’s essential
for understanding kidney function and disorders.
7.
Kidney Function Parameters
1.GlomerularFiltration Rate (GFR):
• Definition: The rate at which the glomerulus filters plasma to form
ultrafiltrate (which later becomes urine).
• Normal Value: ≈120 mL/min.
• Significance: Reflects the kidney’s ability to filter blood and is used to
assess kidney function.
2.Renal Plasma Flow (RPF):
• Definition: The volume of plasma that flows through the kidneys per
minute.
• Normal Value: Approximately 25% of the total cardiac output.
3.Filtration Fraction (FF):
• Definition: The fraction of renal plasma flow that is filtered by the
glomeruli.
• Formula: FF = GFR / RPF.
• Expressed: As a percentage.
8.
8
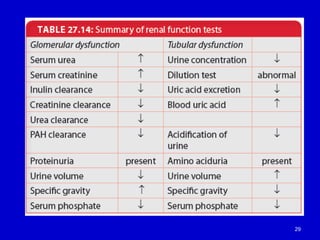
Renal Function Tests
1.To identify renal dysfunction
2. To diagnose renal diseases
3. To monitor disease progress
4. To monitor response to treatment
5. To assess changes in function that may impact
on therapy (e.g. Digoxin, chemotherapy)
9.
Renal Clearance
• Definition:
•Clearance is the volume of blood or plasma completely cleared of a
substance per unit of time.
• Units:
• Expressed in milliliters of plasma per minute (mL/min).
• Function:
• Clearance estimates the amount of plasma that must have passed
through the glomeruli per minute for complete removal of a substance
to account for the substance’s presence in the urine.
• Clinical Relevance:
• Helps assess the kidney’s ability to remove substances from the
plasma and plays a crucial role in determining renal function.
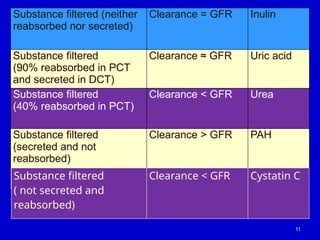
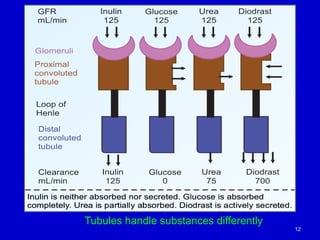
Substance filtered (neither
reabsorbednor secreted)
Clearance = GFR Inulin
Substance filtered
(90% reabsorbed in PCT
and secreted in DCT)
Clearance ≈ GFR Uric acid
Substance filtered
(40% reabsorbed in PCT)
Clearance < GFR Urea
Substance filtered
(secreted and not
reabsorbed)
Clearance > GFR PAH
11
Substance filtered
( not secreted and
reabsorbed)
Clearance < GFR Cystatin C
Inulin Clearance Test
•Purpose:
• Inulin clearance is used to estimate the Glomerular Filtration Rate (GFR).
• Inulin is a polysaccharide that is neither secreted nor reabsorbed by the renal
tubules, making it ideal for GFR measurement.
• Method:
• The amount of inulin filtered from plasma equals the amount recovered in urine:
• Plasma concentration (P) x GFR = Urine concentration (U) x Urine flow rate (V)
• Formula for GFR:
• GFR = (U x V) / P
• U: Urinary concentration of inulin.
• V: Urine flow rate.
• P: Plasma concentration of inulin.
• Normal Values:
• Average GFR:
• 120 mL/min for men
• 100 mL/min for women
• Clinical Relevance:
• Inulin clearance is used as a precise measurement of GFR and renal function.
14.
Creatinine Clearance Test
•Purpose:
• Creatinine clearance is used as a practical method for estimating Glomerular Filtration
Rate (GFR) in clinical practice, as inulin administration is impractical.
• Why Creatinine?:
• Creatinine is a byproduct of skeletal muscle phosphocreatine.
• It is filtered by the kidneys and has a clearance rate similar to that of inulin, making it
useful for GFR estimation.
• Method:
• Formula for Creatinine Clearance:
• Creatinine Clearance = (Urine concentration of creatinine x Urine volume) / Serum
creatinine concentration
• Steps:
• Measure creatinine concentration in a serum sample.
• Collect 24-hour urine and measure the urine creatinine concentration.
• Calculate urine excretion rate by dividing the urine volume by the collection time.
• Clinical Relevance:
• This is a widely used and practical test for assessing kidney function.
• It provides an estimate of GFR based on the clearance of creatinine.
15.
Creatinine Clearance andIts Relationship with GFR
• Creatinine Clearance Calculation:
• Formula:
• Creatinine Clearance=(U×V)P)Where:
• U = Urine concentration of creatinine (mg/dL or mmol/L)
• V = Urine volume (mL/min)
• P = Serum creatinine concentration (mg/dL or mmol/L)
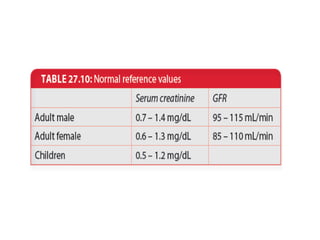
• Normal Serum Creatinine Range:
• Serum creatinine concentration: 20-80 mmol/L (0.28-0.90 mg/dL)
• GFR and Serum Creatinine Relationship:
• An increase in serum creatinine indicates decreased GFR.
• When GFR decreases by 50%, serum creatinine concentration doubles.
• Clinical Significance:
• A rising serum creatinine level is a key indicator of renal impairment.
• Creatinine clearance provides an estimate of renal function, helping
assess kidney health and the extent of renal damage.
16.
Procedure for CreatinineClearance Test
1.Hydration:
• Administer 500 mL of water to the patient to promote urine flow.
2.Initial Urine Collection:
• After 30 minutes, ask the patient to empty their bladder and
discard the urine.
3.Timed Urine Collection:
• Exactly 60 minutes later, collect the urine sample.
• Note the urine volume collected during this period.
4.Blood Sample:
• Take a blood sample to measure the serum creatinine level.
5.Testing and Calculation:
• Measure creatinine concentration in both the blood and urine
samples.
• Use the formula to calculate creatinine clearance.
Urea Clearance inKidney Function
• Definition:
• Urea clearance is the volume of blood that is cleared of urea by the kidneys per minute.
• Formula:
• Urea Clearance (Curea) = U×V/P
• U = Concentration of urea in urine (mg/ml)
• V = Volume of urine excreted per minute (ml/min)
• P = Concentration of urea in plasma (mg/ml)
• Factors Influencing Urea Clearance:
• Reabsorption: About 40% of urea is reabsorbed by renal tubules after filtration, which makes urea
clearance highly dependent on urine flow rate.
• Hydration Status:
• In hydrated states, urine flow is high and urea clearance may be >70% of GFR.
• In dehydrated states, urea clearance may be <30% of GFR.
• Maximum Urea Clearance:
• The reference range is 60-100 ml/min.
• Clinical Relevance:
• Curea is not useful for direct estimation of GFR due to the significant reabsorption of urea.
• Hydration and urine flow must be taken into account for accurate interpretation.
21.
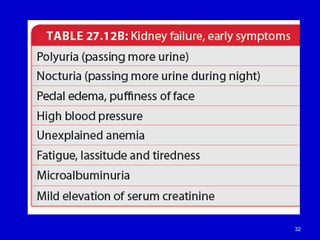
Serum Urea andCreatinine in Renal Failure
• Key Tests:
• Serum Urea and Creatinine are first-line tests in diagnosing renal failure.
• These tests are used to assess kidney function and glomerular filtration rate (GFR).
• Renal Failure and Lab Results:
• Decreased Urine Volume:
• Renal failure leads to reduced urine output (oliguria or anuria).
• Creatinine Clearance:
• Creatinine clearance decreases as kidney function deteriorates.
• Creatinine levels in blood increase due to impaired filtration.
• Increased Serum Urea:
• As kidney function declines, the reabsorption of urea increases, leading to elevated serum
urea levels.
• Clinical Implications:
• Elevated serum creatinine and urea levels indicate impaired kidney function and
reduced glomerular filtration rate (GFR).
• These biomarkers help in diagnosing acute and chronic renal failure.
22.
Cystatin C asa Marker of GFR
• Overview:
• Cystatin C is a 122-amino acid protein (13 kDa) that acts as a cysteine proteinase
inhibitor.
• It is produced by all nucleated cells at a constant rate via a housekeeping gene.
• Filtration and Metabolism:
• Freely filtered through the glomerulus due to its small size and basic isoelectric point.
• Not secreted by renal tubules.
• After filtration, cystatin C is catabolized in the renal tubules, preventing its return to plasma.
• Advantages for GFR Estimation:
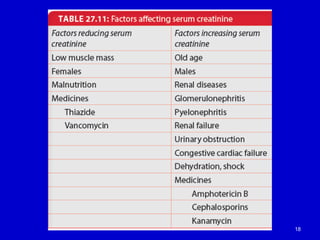
• Cystatin C concentration is not affected by age, unlike creatinine, which tends to increase
with age due to muscle mass changes.
• More reliable marker of GFR, especially in cases where creatinine may be influenced by
muscle mass, diet, or other factors.
• Limitations:
• Inflammatory conditions or other non-GFR-related factors can affect cystatin C levels.
• Though a good marker, cystatin C is influenced by conditions like inflammation or stress.
• Clinical Utility:
• A valuable alternative to serum creatinine for estimating glomerular filtration rate (GFR).
• Can be particularly useful in situations where creatinine levels might be misleading (e.g., in
elderly patients or those with altered muscle mass).
23.
Water dilution test
Procedure:
1- the subject evacuates his bladder and then
drinks 1.5 liters of water.
2- urine is collected from the bladder every one
hour for 5 hours .
3- volume and specific gravity of each sample is
determined.
23
24.
Normal values :
Volume:
More than 800 ml
Specific gravity :
Below 1.010
Abnormal values :
Specific gravity doesn’t fall below 1.010
(due to impaired function of distal tubules)
24
25.
Water concentration test
Procedure:
1- the subject evacuates his bladder and is
then prevented from taking fluids for 10-12
hours to produce dehydration.
2- at the end of 12 hours a urine sample is
taken and the specific gravity is measured.
25
26.
Normal value :
Specificgravity :
More than 1.025
Abnormal value :
Specific gravity remains below 1.020
(due to impairment in the function of loop of
henle and distal tubules)
26
27.
Renal Plasma Flow(RPF) and PAH Clearance
• Overview of RPF:
• Renal Plasma Flow (RPF) is the volume of plasma that flows through the kidneys per minute.
• Normal range: 600-700 mL/min for an adult.
• Measurement with PAH:
• PAH (Para-aminohippuric acid) is a substance that is used to estimate renal plasma flow.
• 90% of PAH is removed by the kidneys through both glomerular filtration and tubular secretion.
• This high extraction rate allows for an accurate measurement of effective renal plasma flow
(ERPF).
• PAH Clearance Calculation:
• PAH is infused to maintain a constant plasma concentration.
• The formula used for calculating PAH clearance:
• Clearance of PAH=UPAH×V/PPAH
• Where:
• UPAH= concentration of PAH in urine (mg/mL)
• V = urine flow rate (mL/min)
• PPAH = concentration of PAH in plasma (mg/mL)
• Radionuclides for Estimation:
• Nowadays, Iodine-131 iodohippurate (I-131) or other radionuclides (such as diodrast) are used
to estimate renal plasma flow.
• These methods improve the accuracy of RPF measurement, especially in clinical settings.
• Clinical Significance:
• Estimation of RPF is essential for assessing kidney function and perfusion.
• A decrease in RPF may indicate renal hypoperfusion or vascular abnormalities.
Novel Biomarkers ofTubular Injury
• Neutrophil Gelatinase-Associated Lipocalin (NGAL):
• Urinary NGAL (uNGAL) is one of the most promising
biomarkers for early detection of acute kidney injury
(AKI), even before a change in GFR.
• Kidney Injury Molecule-1 (KIM-1):
• Sensitive to renal tubular injury and can help in
detecting AKI in its early stages.
• Liver Fatty Acid Binding Protein (LFABP):
• Reflects renal tubular damage, particularly after
ischemic injury.
• Interleukin-18 (IL-18):
• A pro-inflammatory cytokine that can indicate early
kidney injury and is useful for diagnosing AKI.
34.
New Biomarkers forKidney Diseases
• Fibroblast Growth Factor-23 (FGF-23):
• Rises with declining kidney function in patients with
Chronic Kidney Disease (CKD).
• Elevated FGF-23 levels are associated with worsening
renal function and mineral bone disorders.
• FGF-23 plays a role in regulating phosphate
homeostasis and vitamin D metabolism.
• Importance:
• Early detection of CKD progression.
• Potential marker for cardiovascular risk in CKD
patients.