Downloaded 274 times

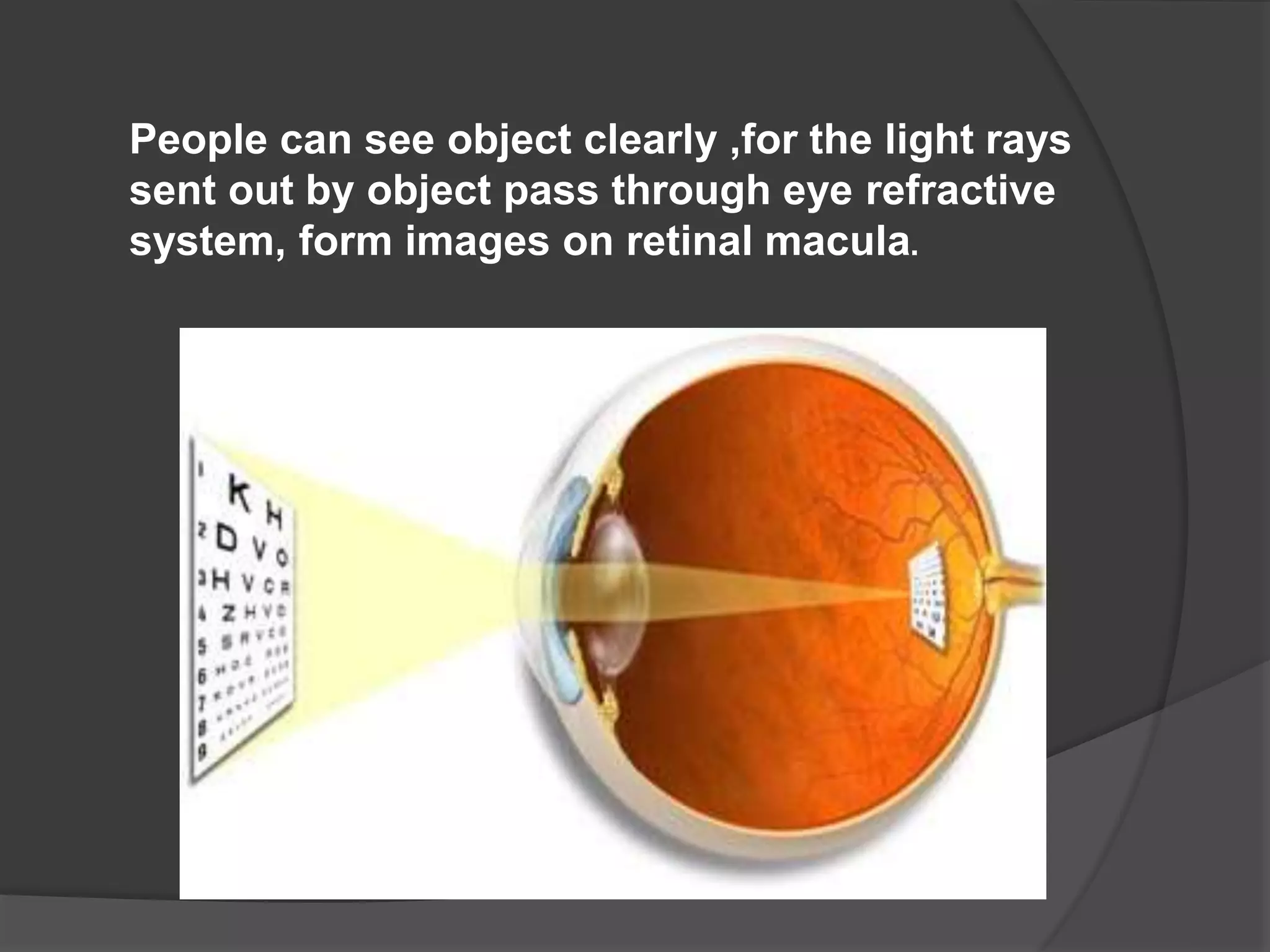




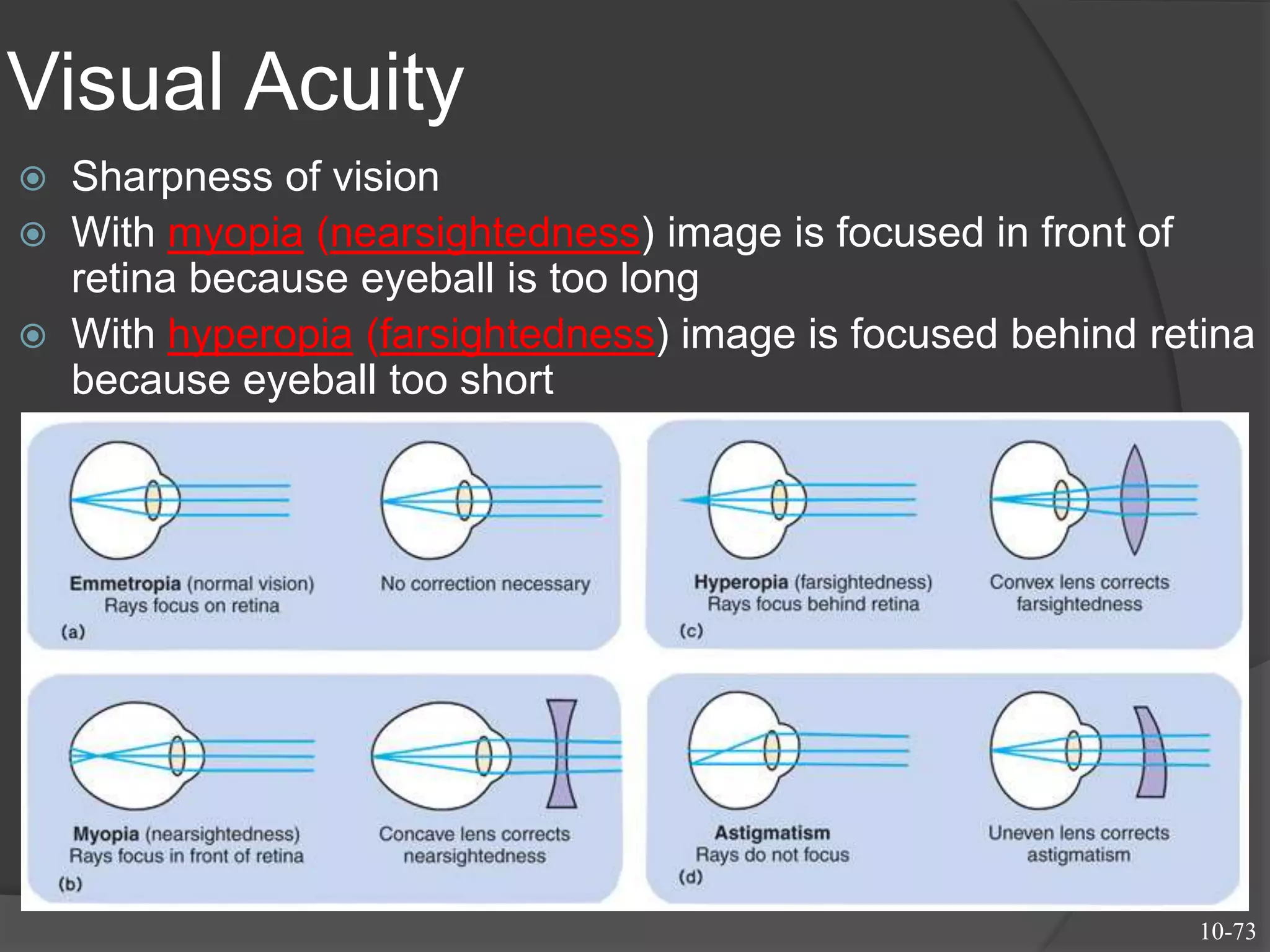




Visual acuity refers to the sharpness and clarity of vision. It is affected by factors like the size and contrast of the object, as well as optical and retinal factors in the eye. The normal visual acuity allows discrimination of objects spaced 1 minute of arc apart. Visual acuity declines in the peripheral vision due to the dense concentration of photoreceptors in the fovea. Common refractive errors that impair visual acuity include myopia, hyperopia, and astigmatism. These errors occur when the eye is not the proper length or shape to focus light correctly on the retina.
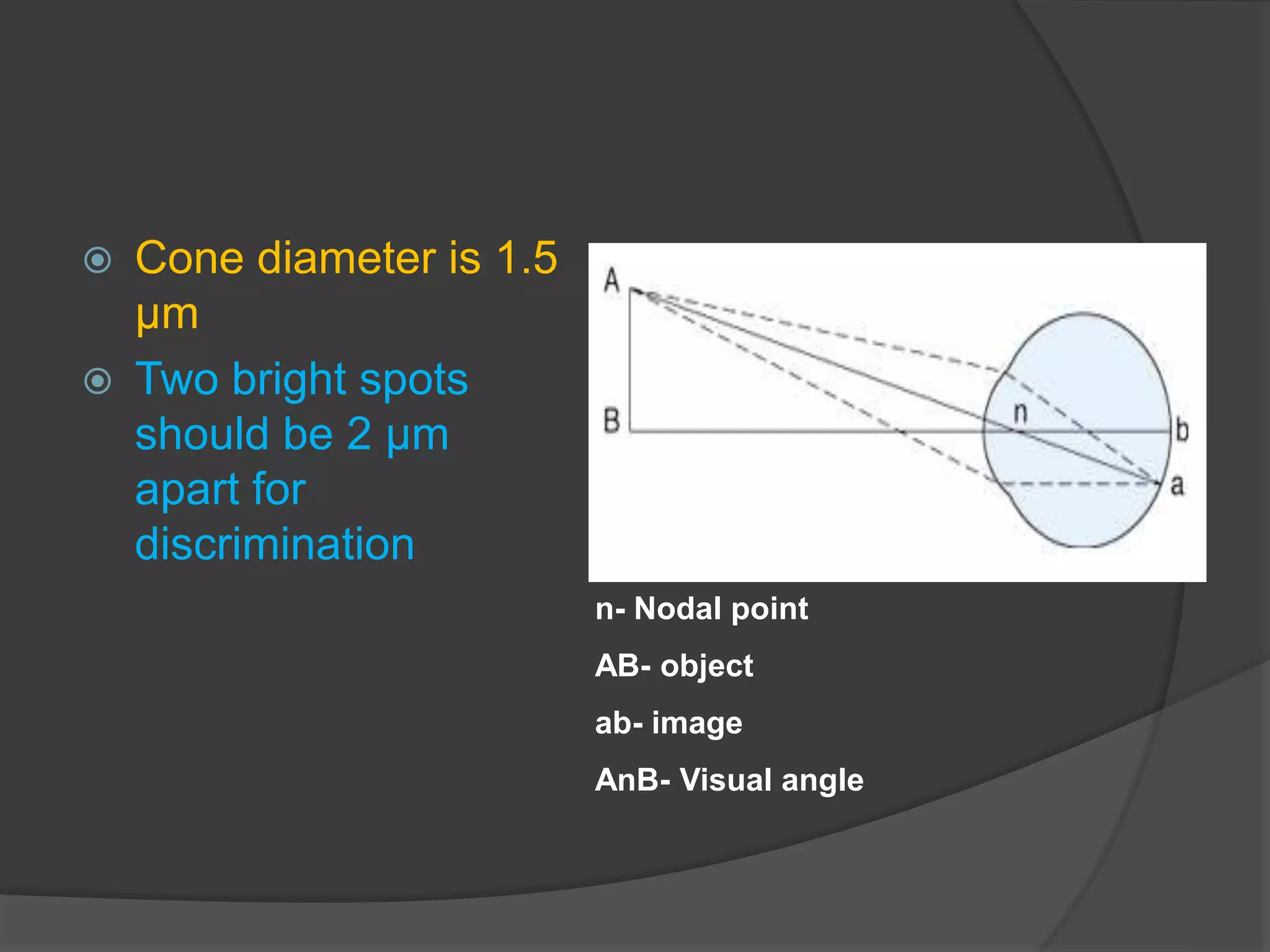
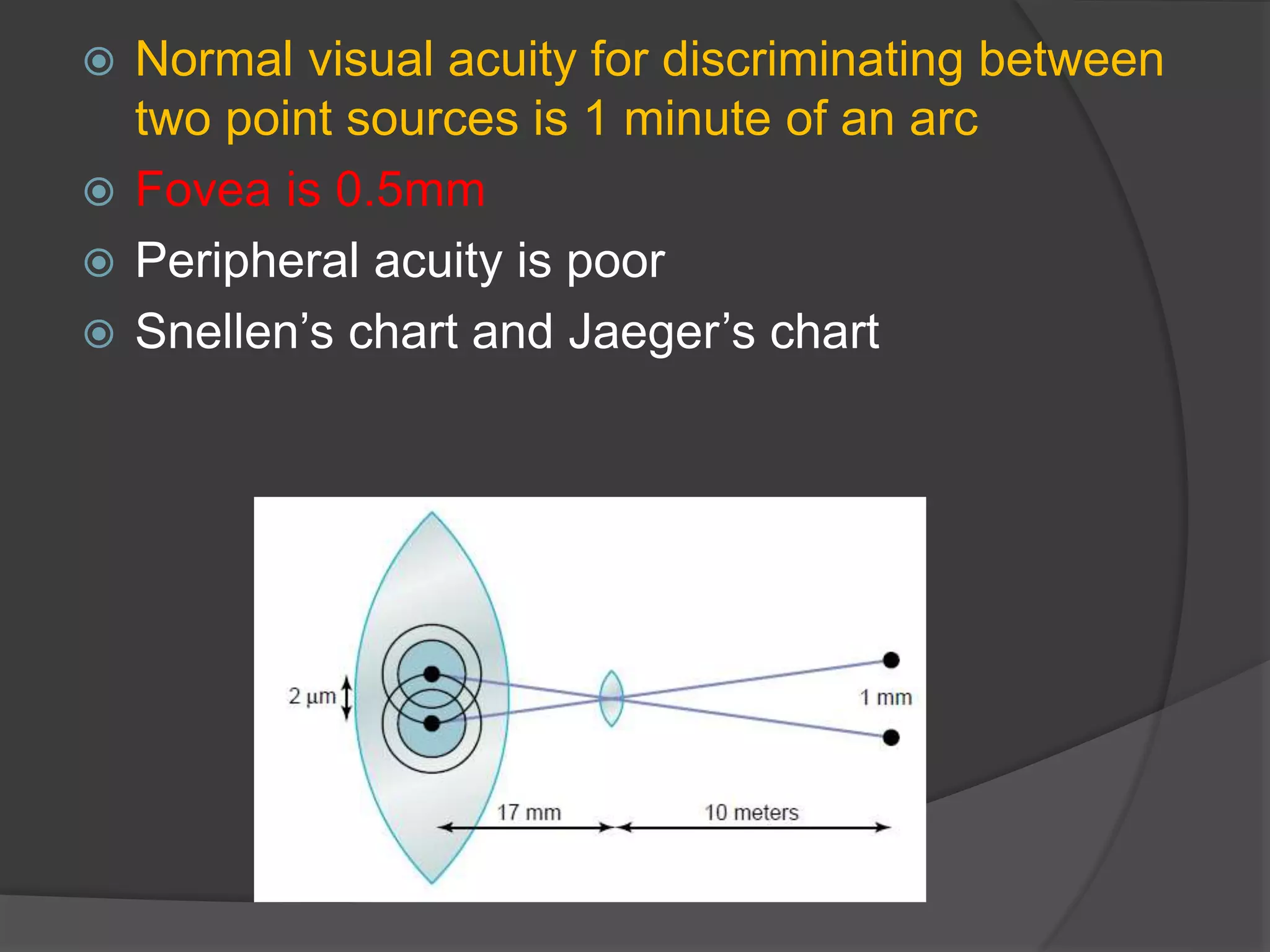
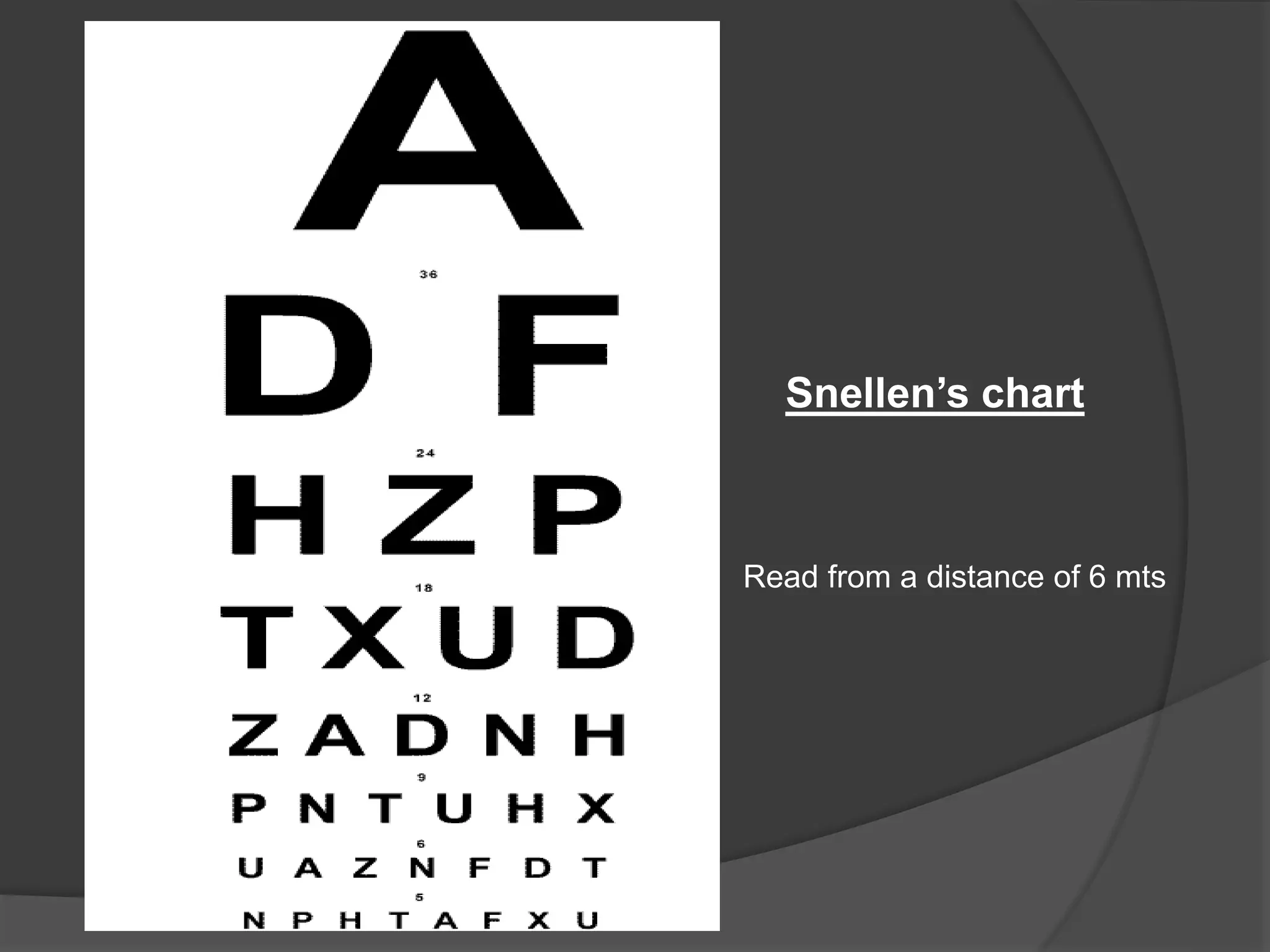
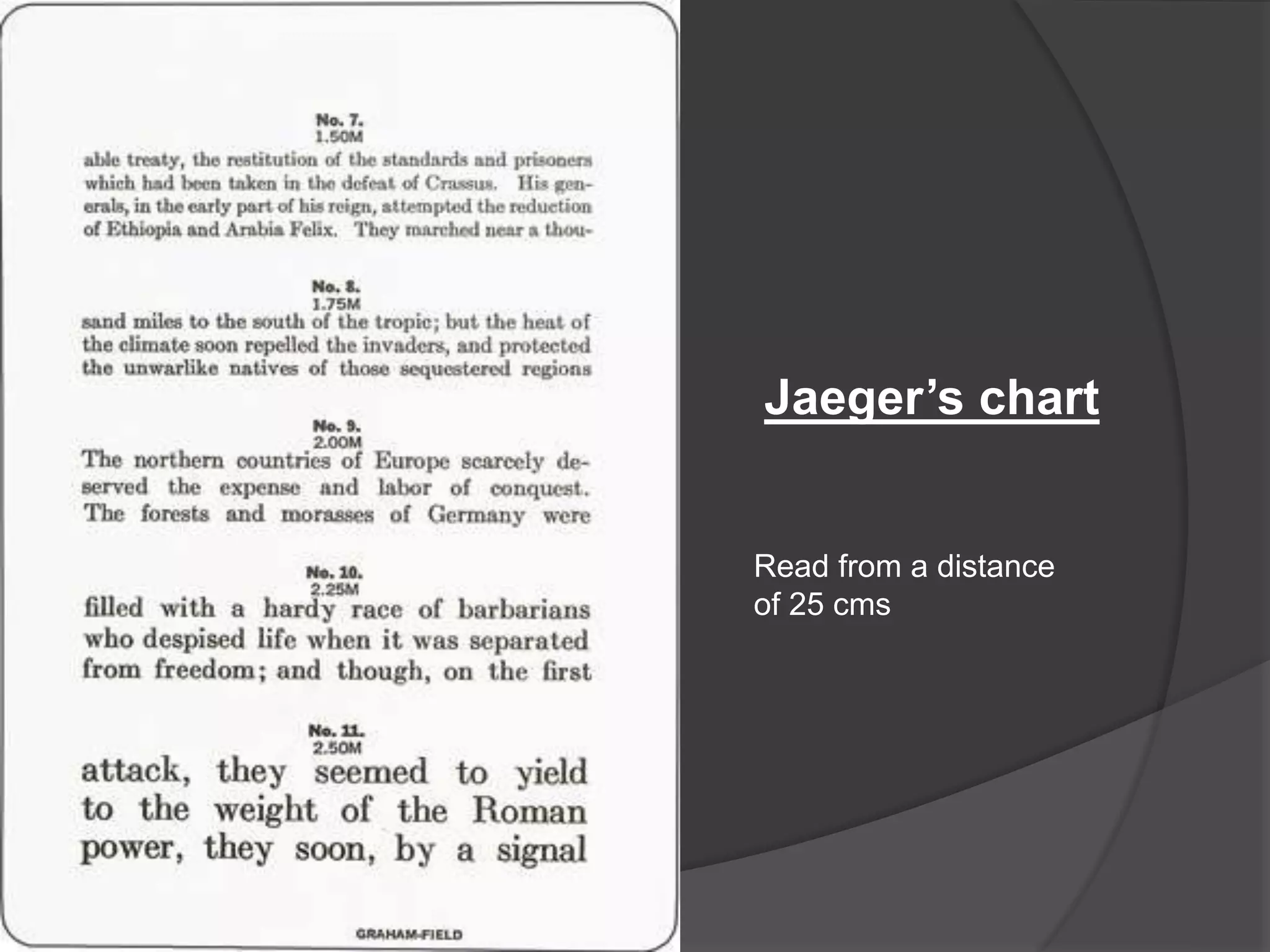
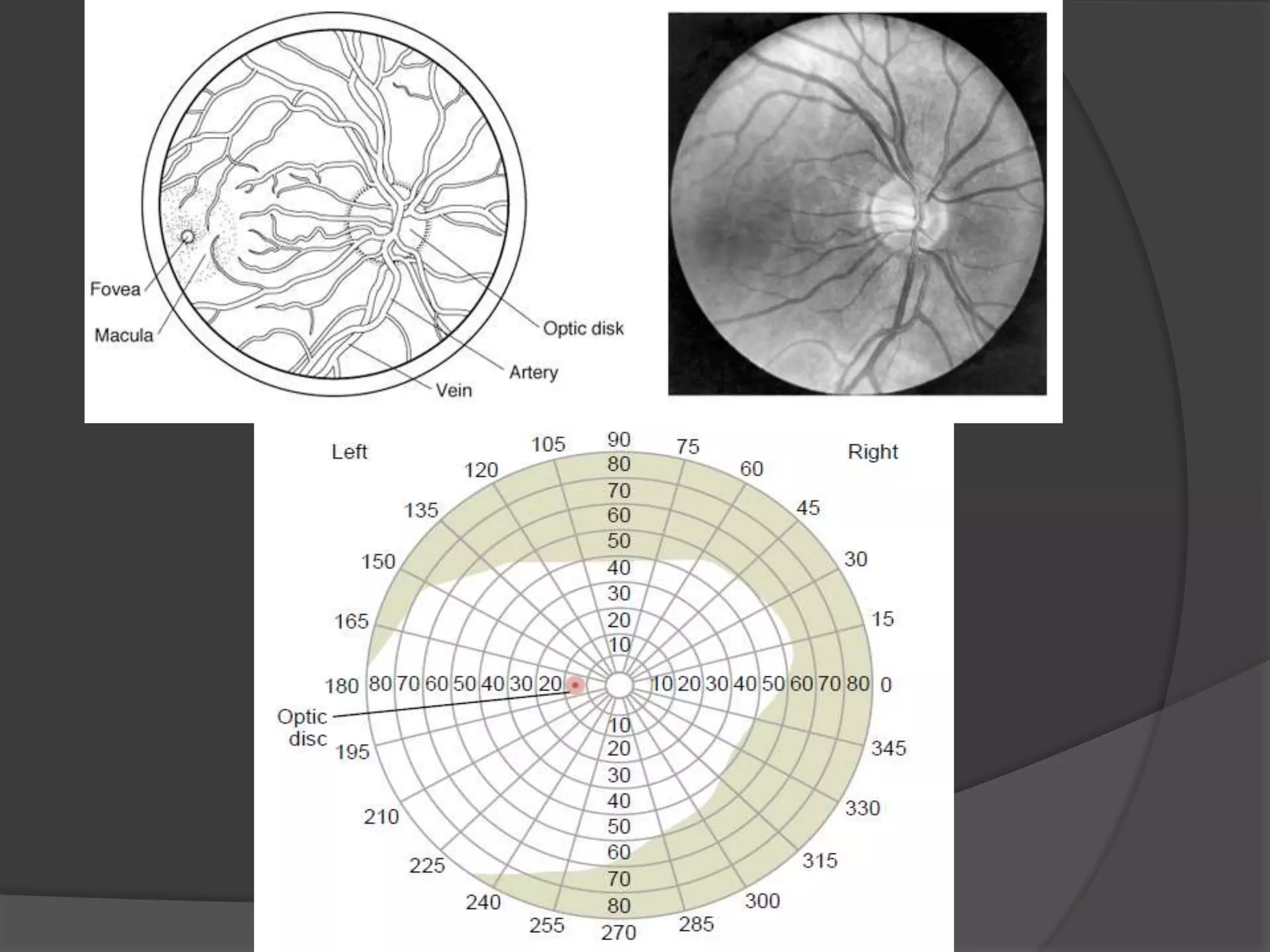
Visual acuity describes detail perception, measured in visual angles. Normal acuity is 1 minute of arc, assessed using Snellen’s and Jaeger’s charts.
Snellen's chart requires reading from 6m; Jaeger’s chart from 25cm. Visual field assessment methods include perimetry and confrontation.
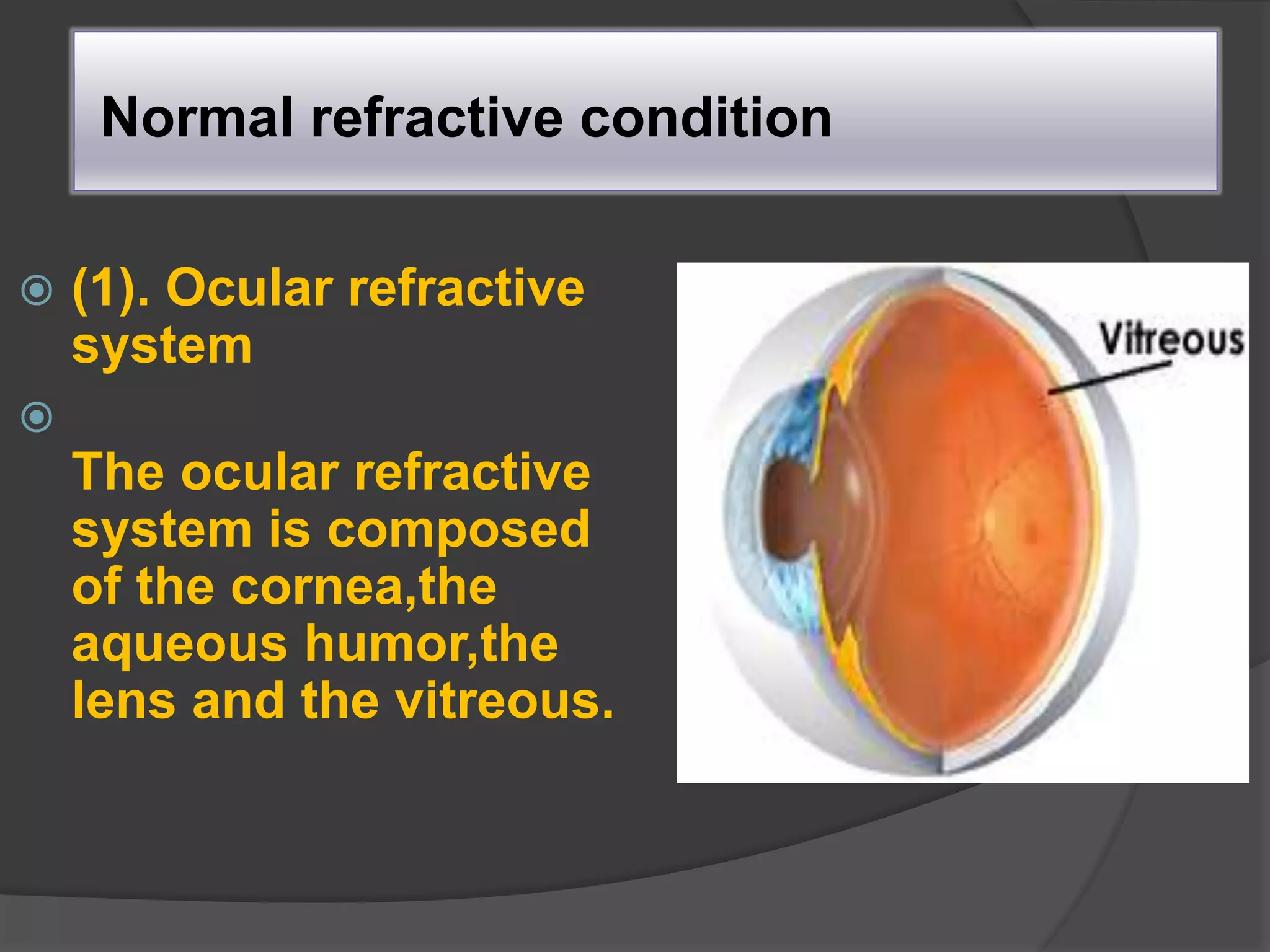
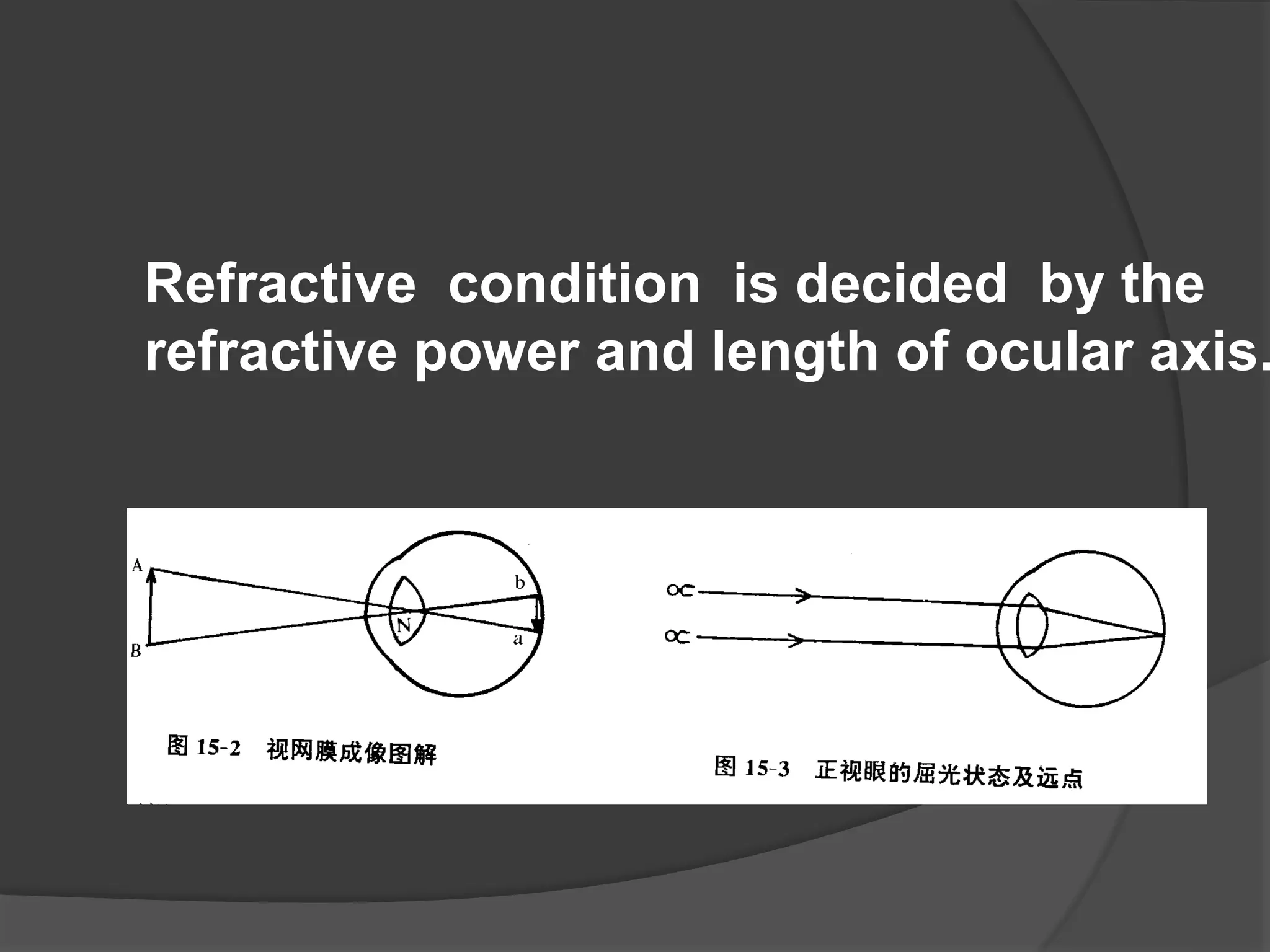
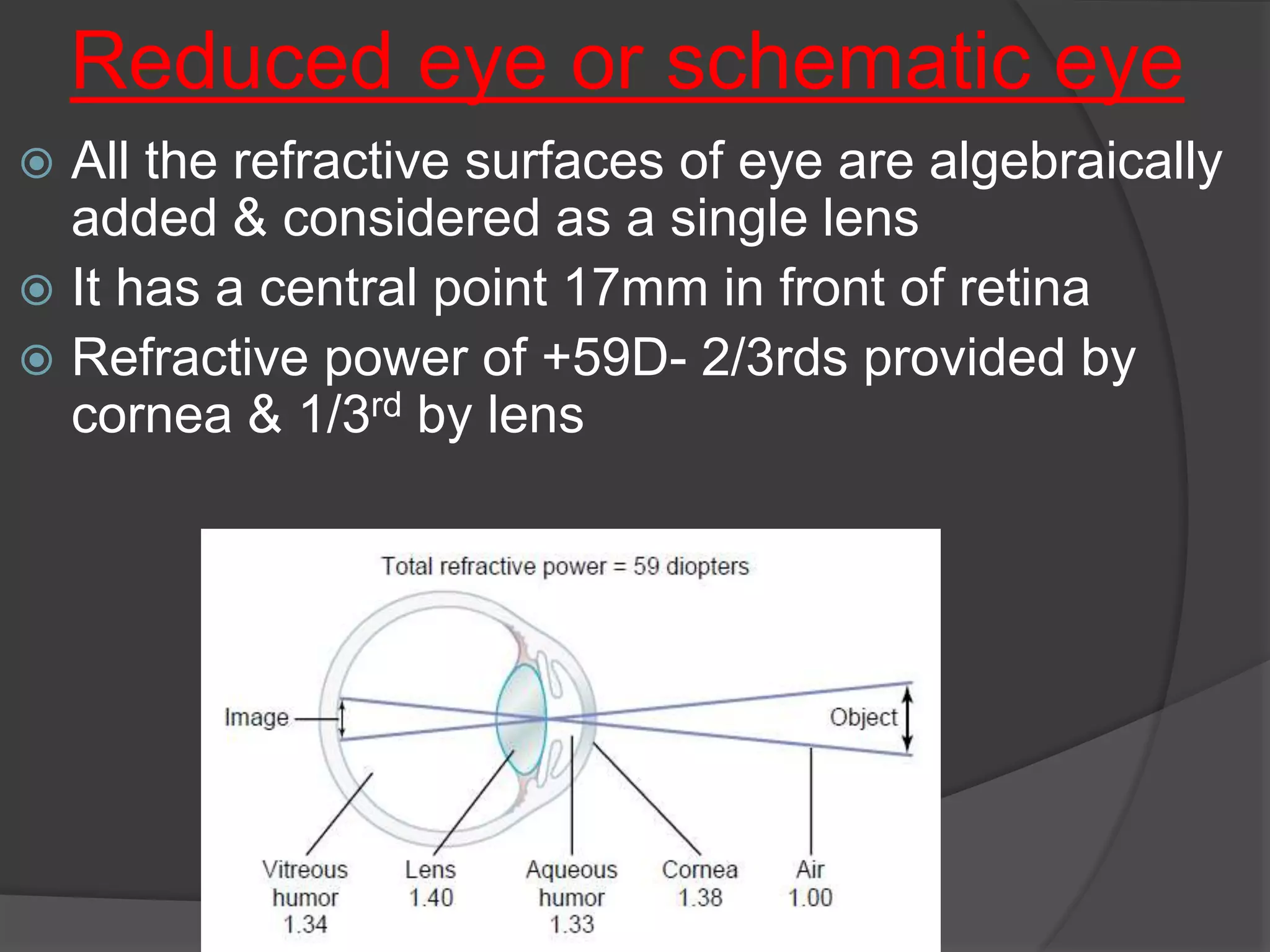
The ocular refractive system includes cornea, aqueous humor, lens, and vitreous. Refractive power and ocular axis length determine refractive condition.
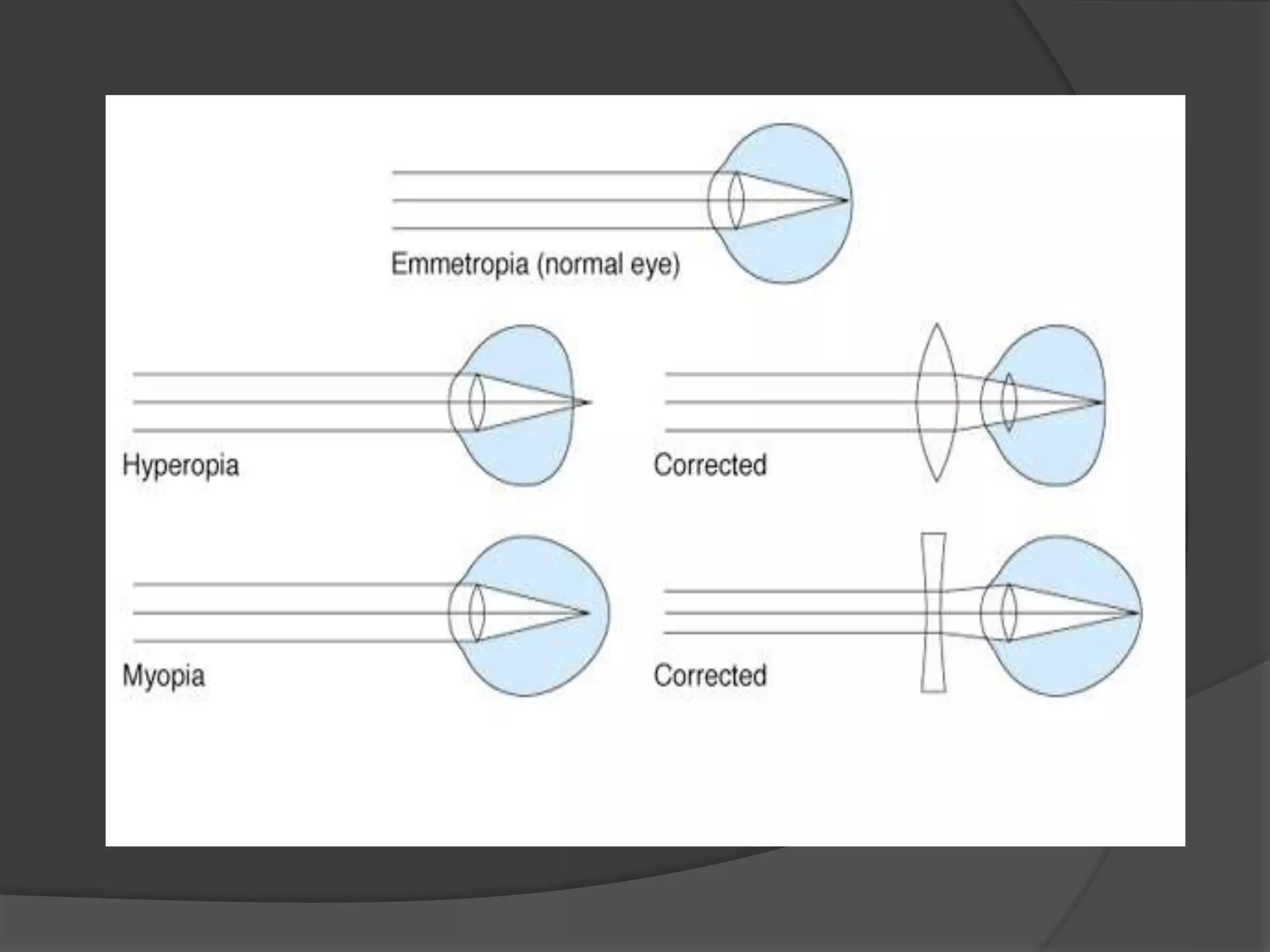
Emmetropia indicates no refractive error. Ametropia denotes misalignment causing focus issues on the retina including myopia, hypermetropia, and astigmatism.
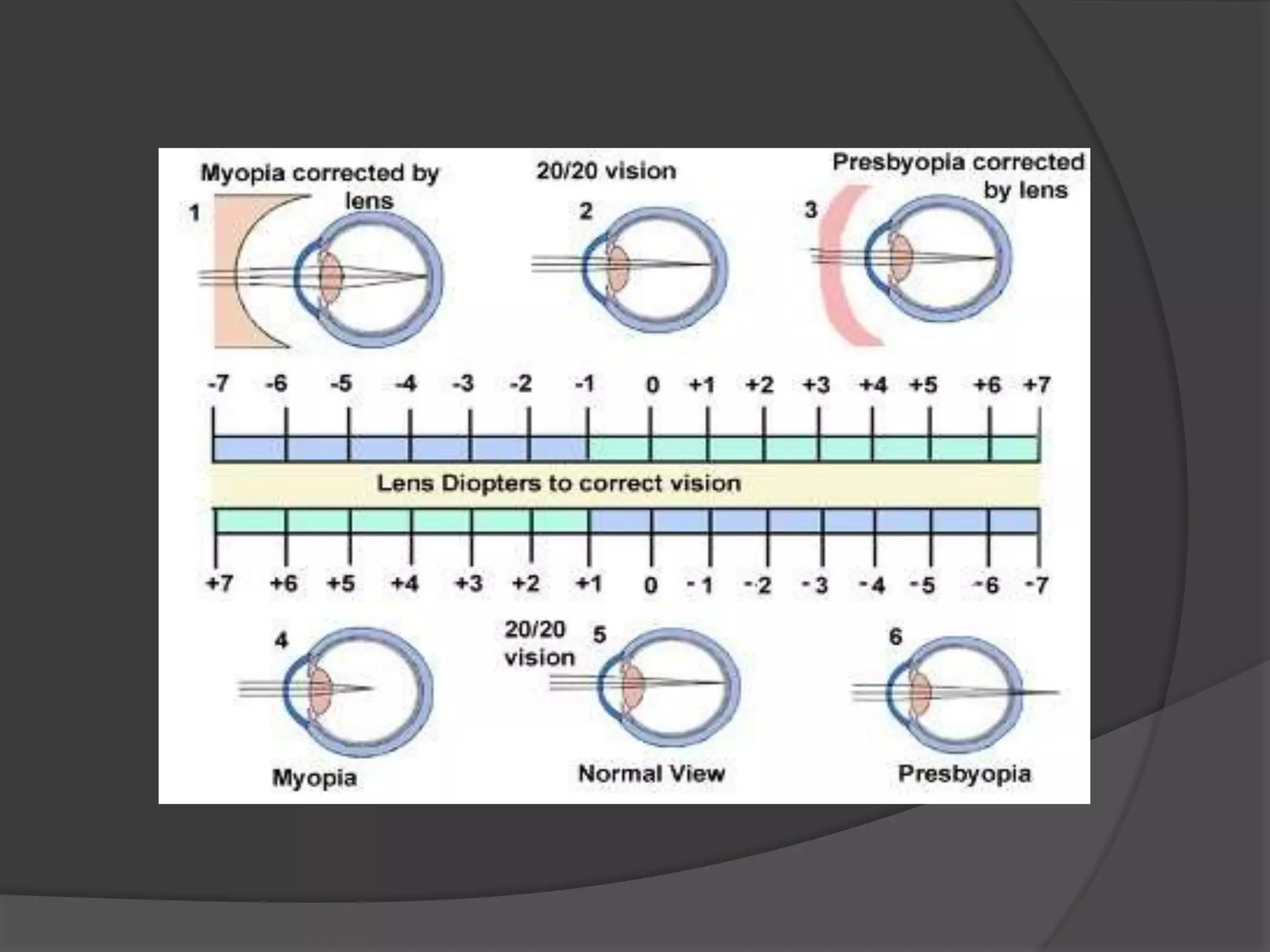
Myopia (nearsightedness), hypermetropia (farsightedness), and emmetropia (normal vision) discussed with correction methods such as lenses.
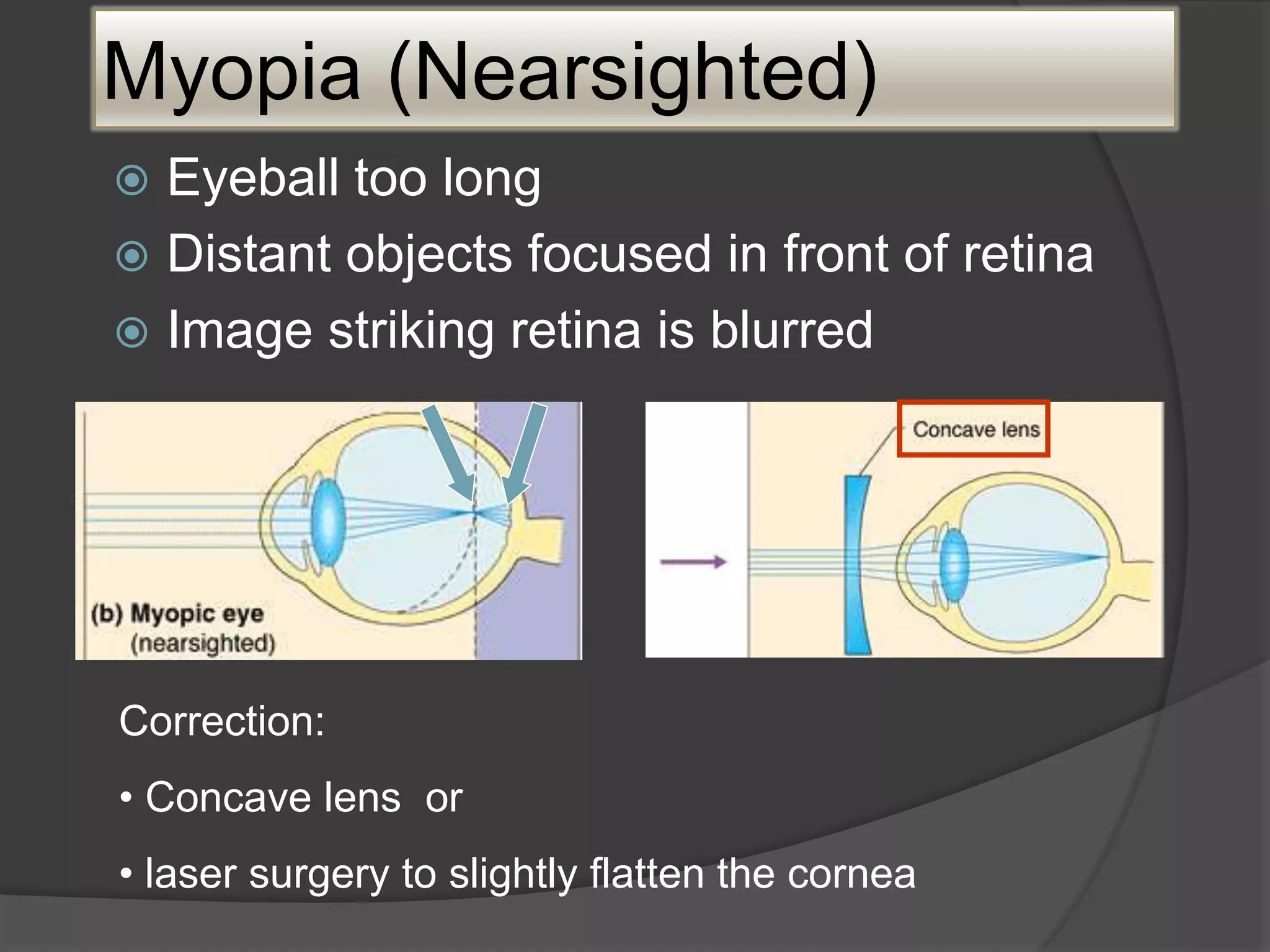
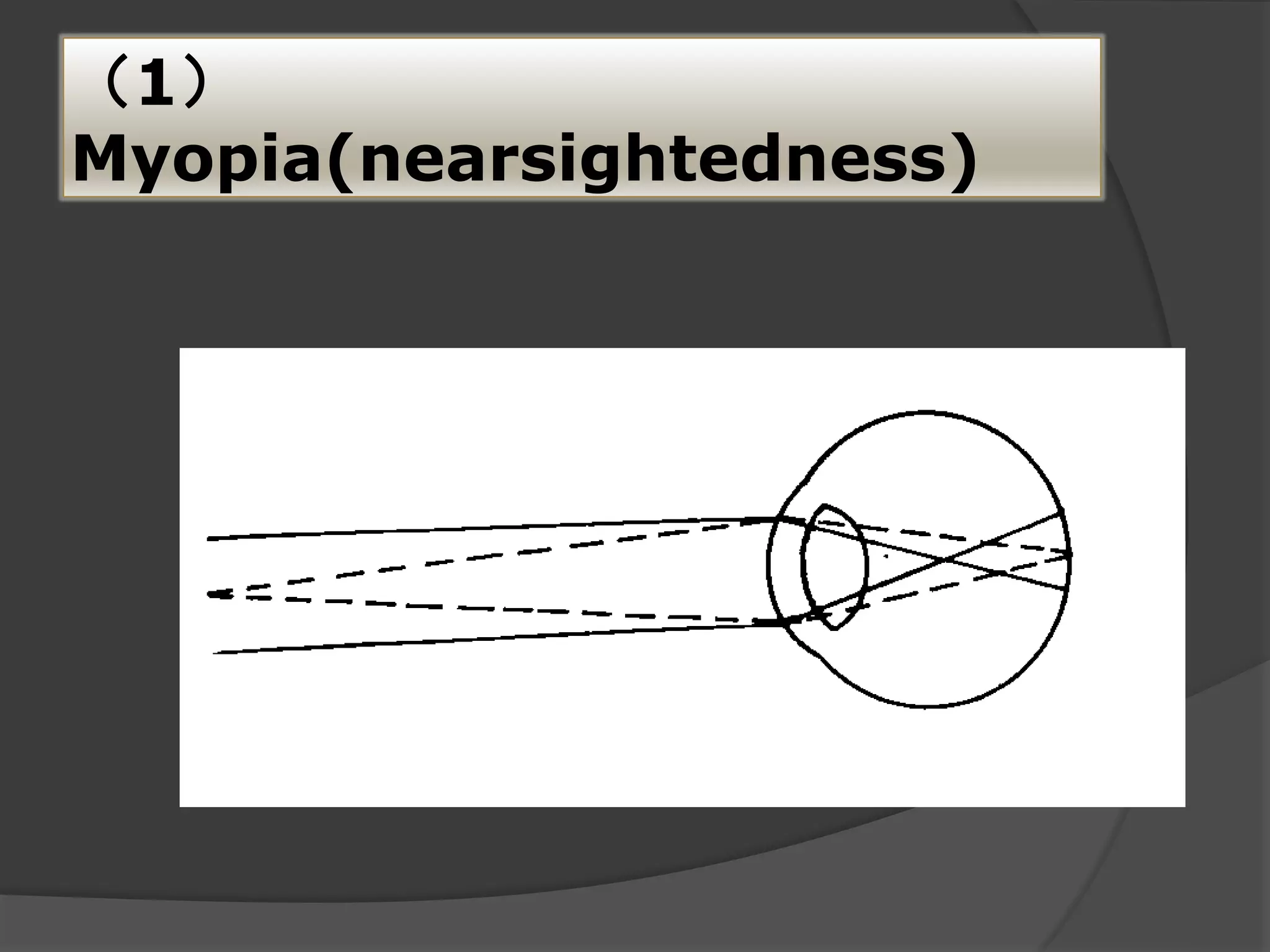
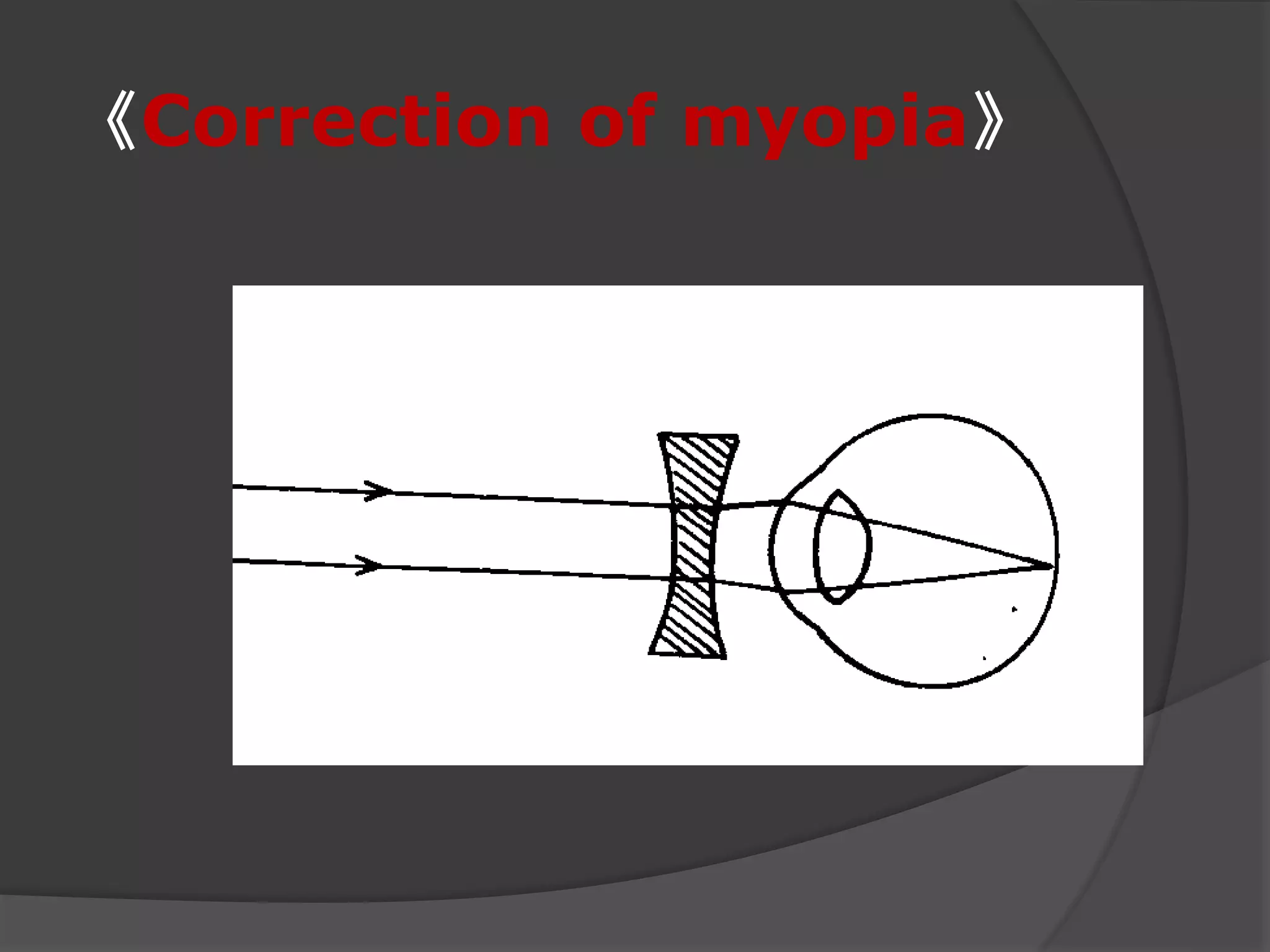
Myopia causes light to focus in front of the retina. Conditions range from mild to high. Corrective options include concave lenses and laser surgery.
Axial myopia: increased length of the eye; Refractive myopia: normal axis with increased refractive power.
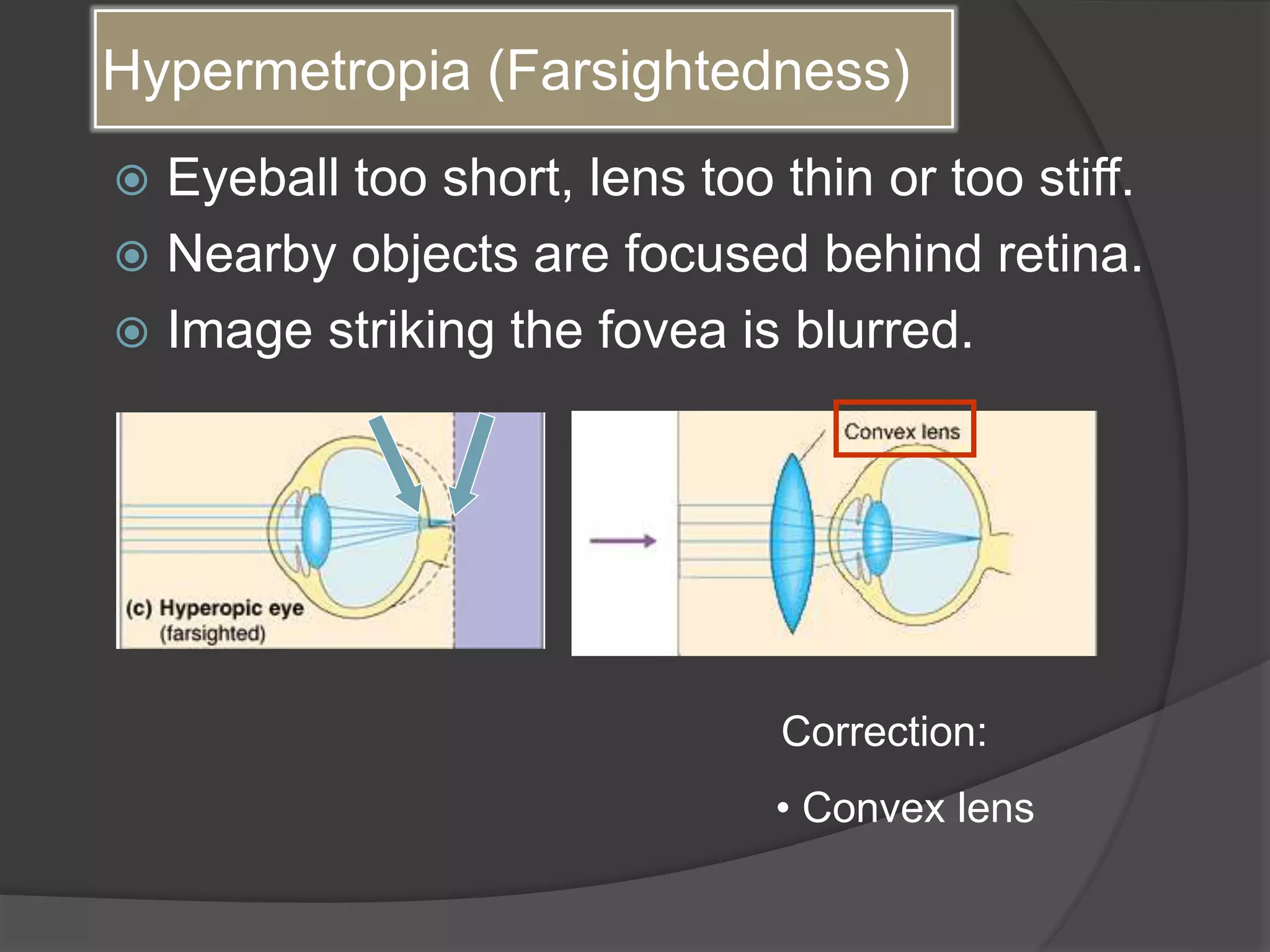
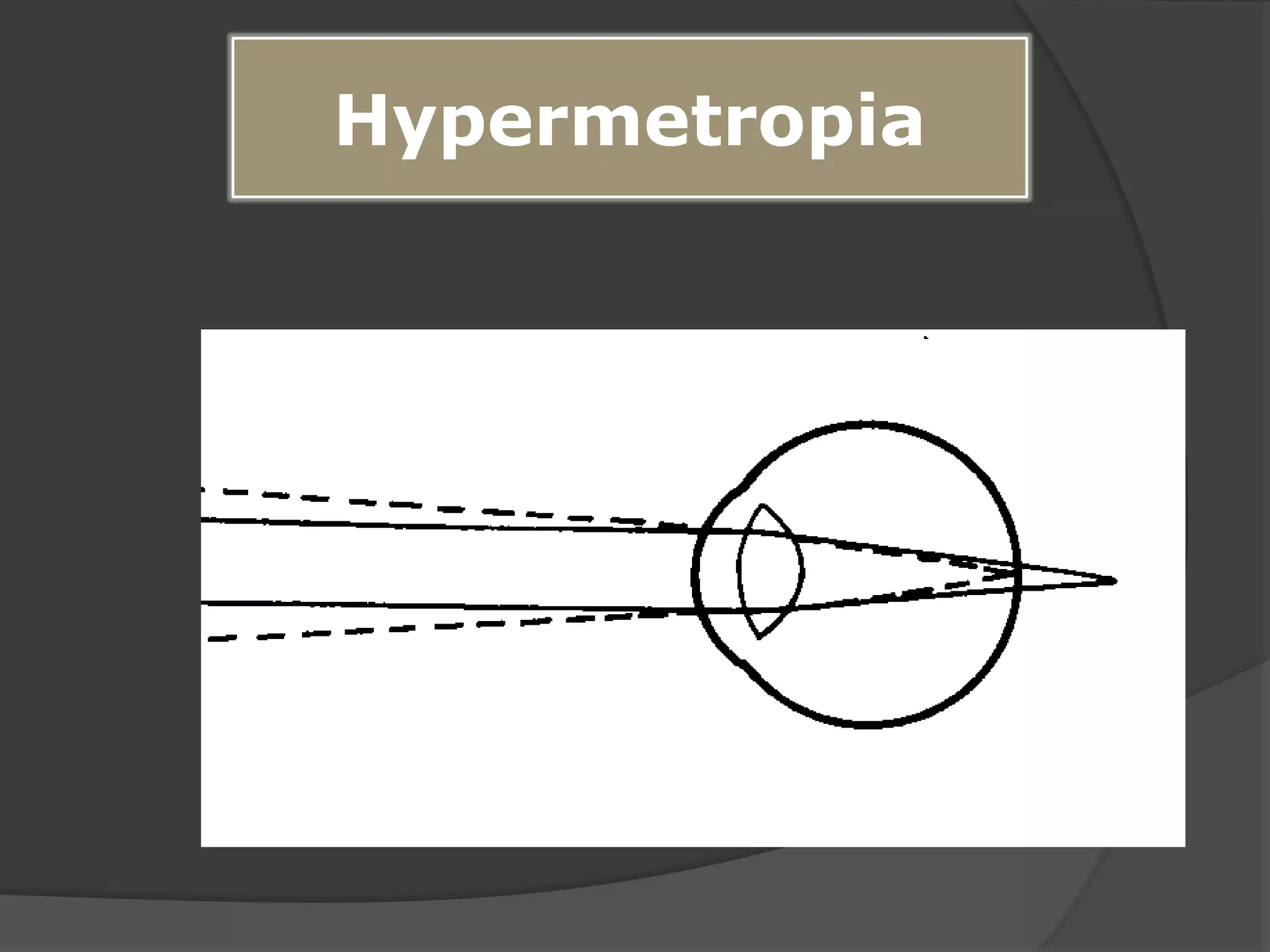
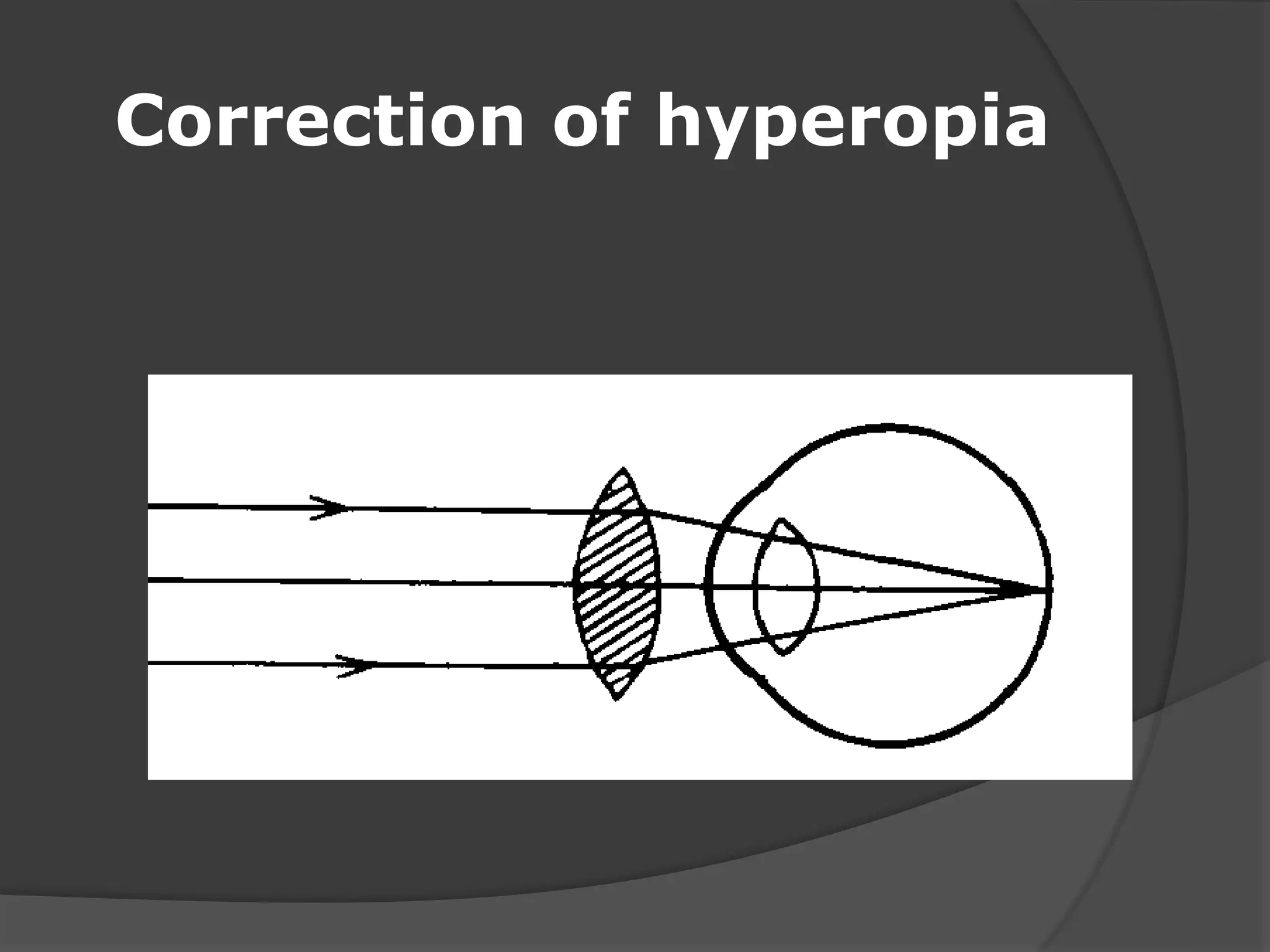
Hypermetropia causes images to focus behind the retina; typically leads to difficulty seeing close objects. Corrected with convex lenses.
Symptoms include blurred vision, eye fatigue, and eye strain. Classified as mild (<+3D), moderate (+5D), or high (>+5D). Etiology details axial and refractive hyperopia.
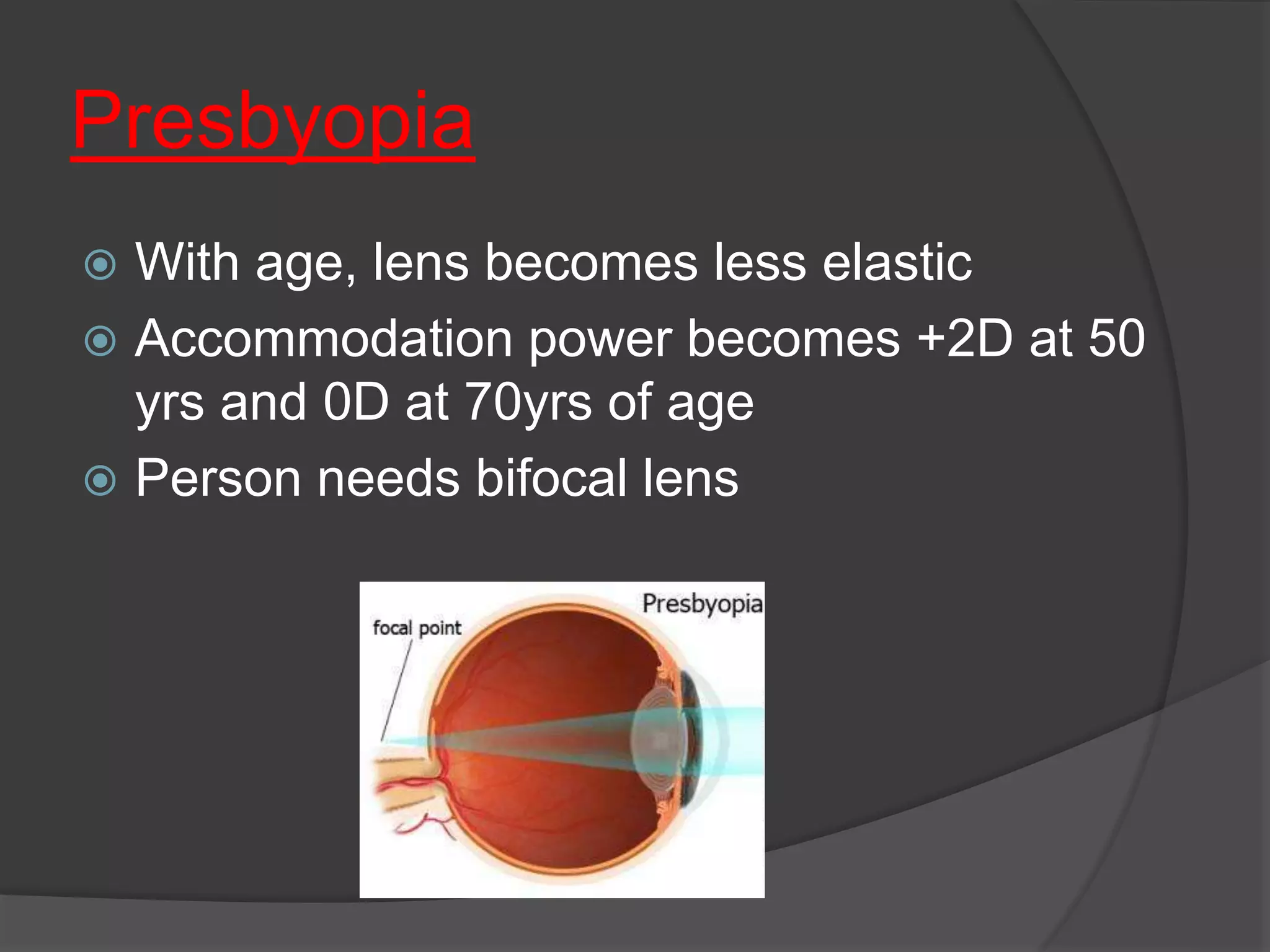
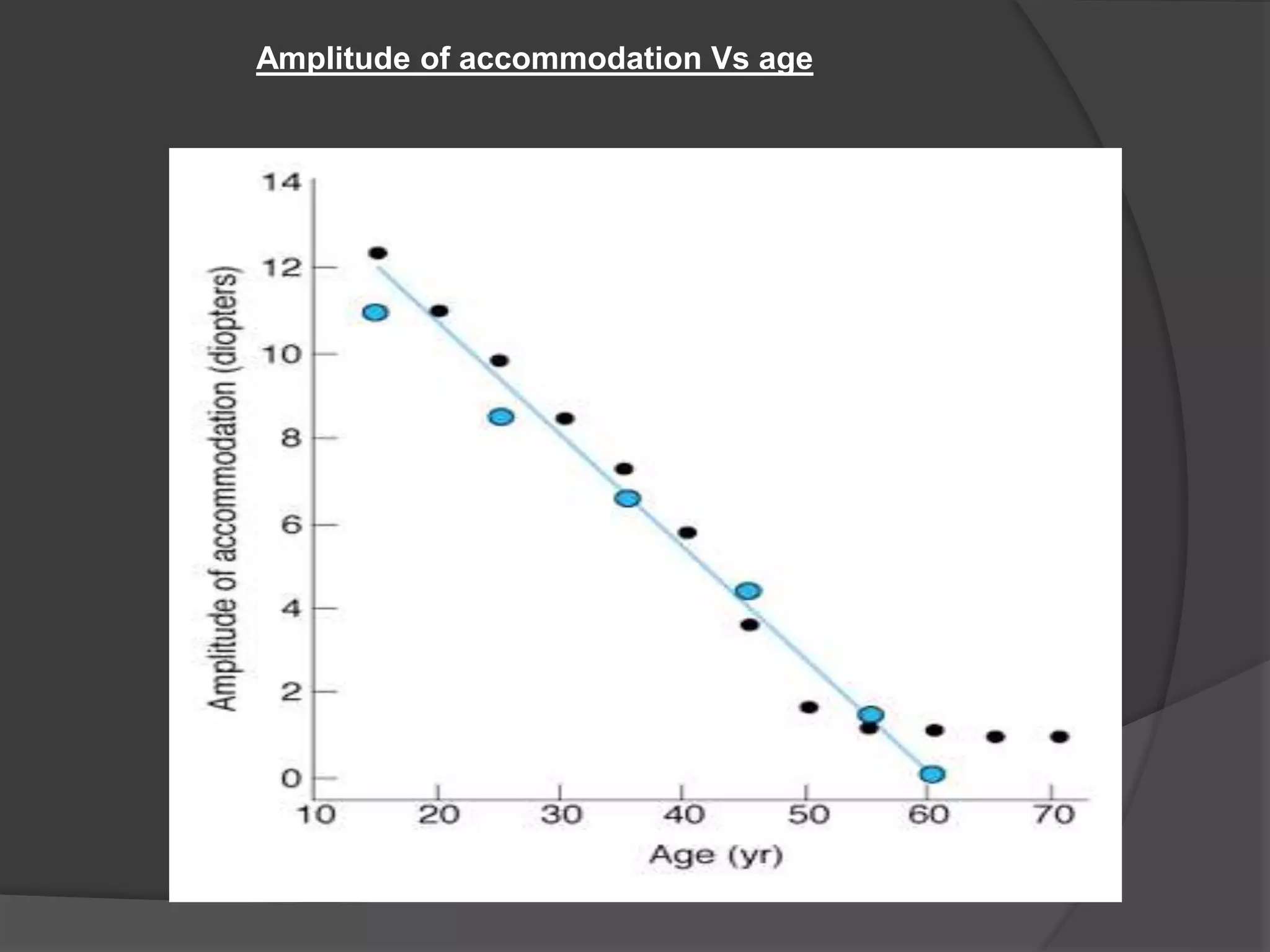
Presbyopia occurs with age, resulting in decreasing lens elasticity and accommodation. Symptoms include difficulty reading fine print.
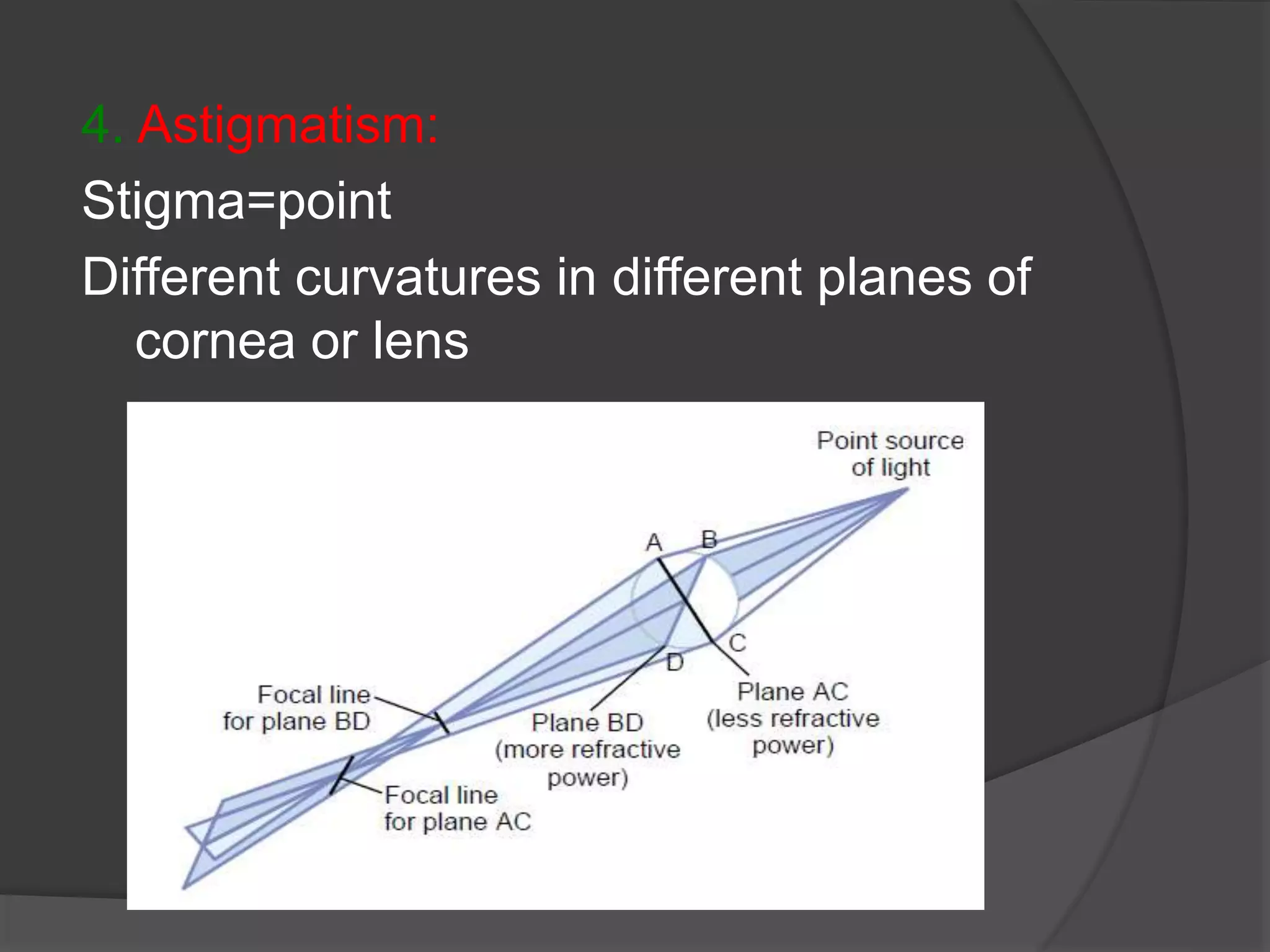
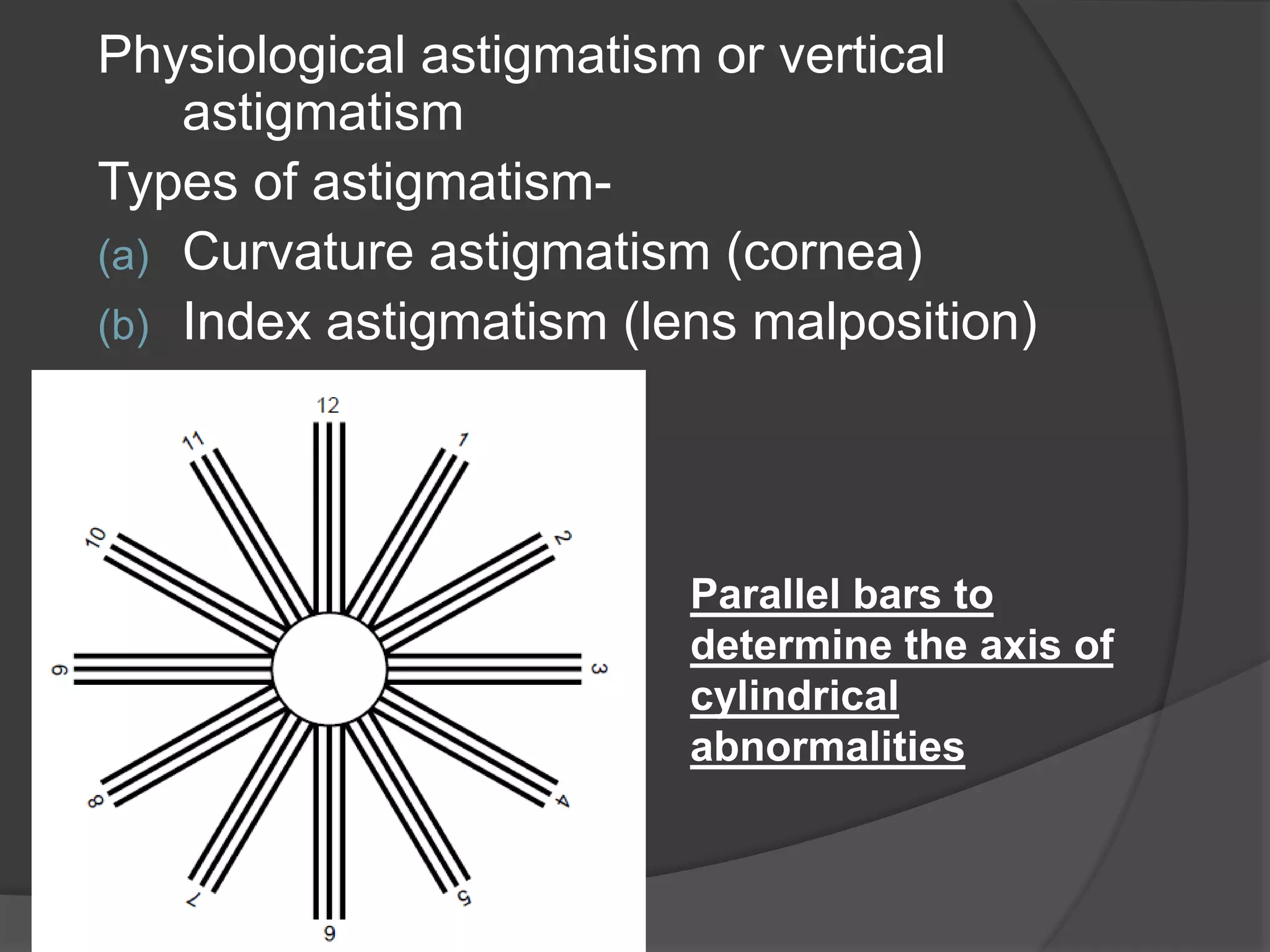
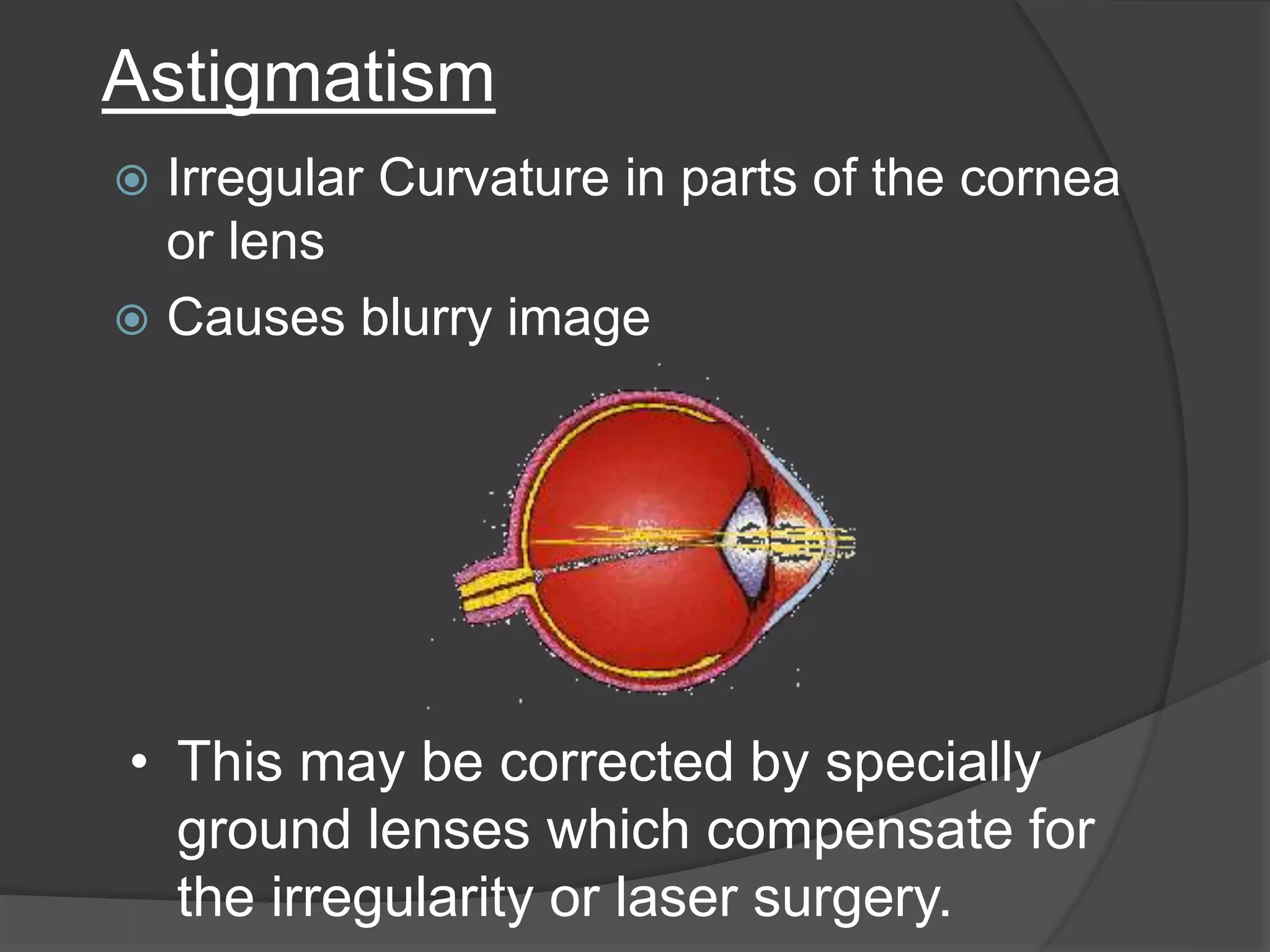
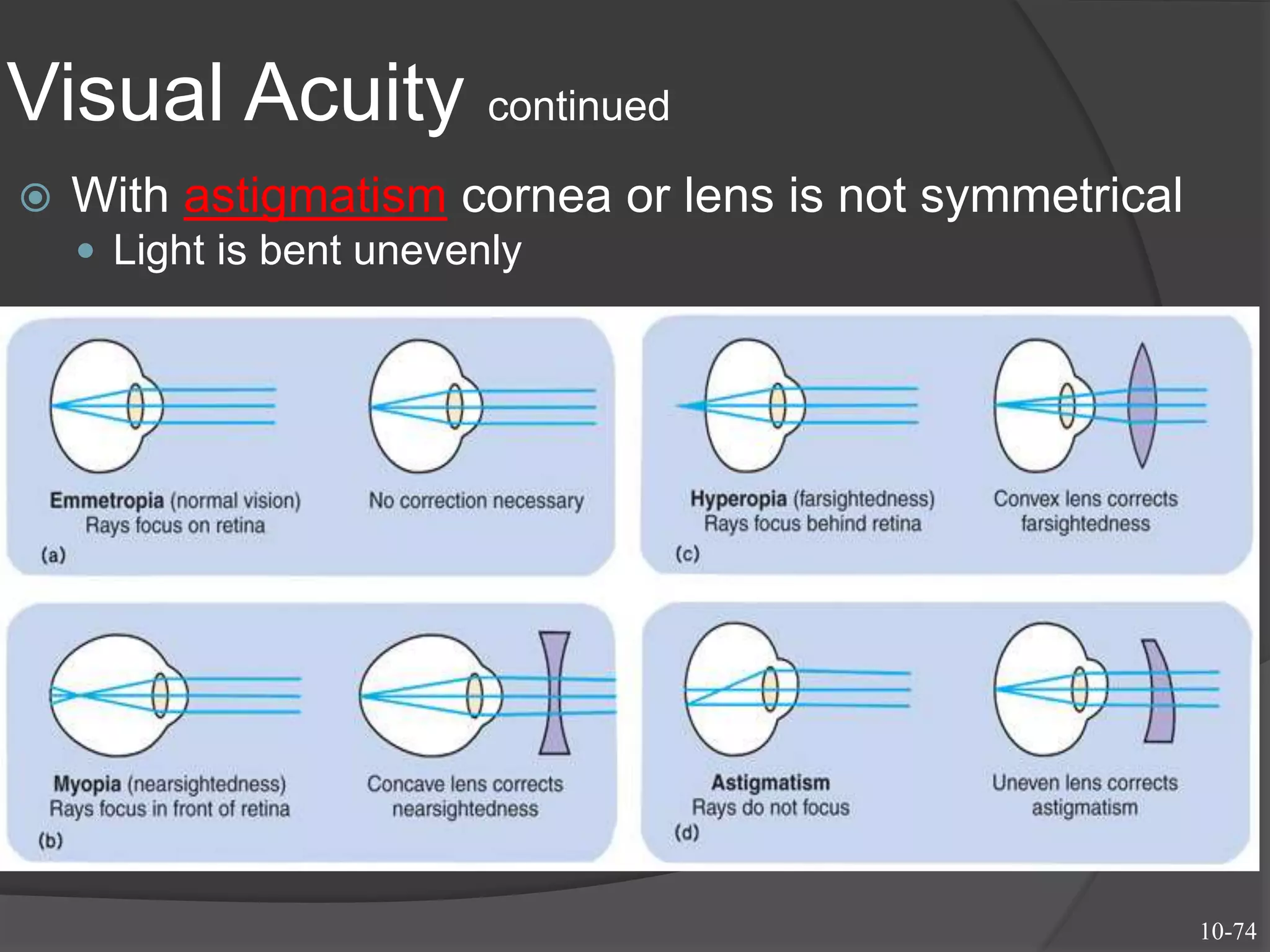
Astigmatism due to uneven refractive power causes blurred vision. Corrective measures include cylindrical lenses or surgical options.
Contact lenses provide broader field of view and do not reduce object size significantly.
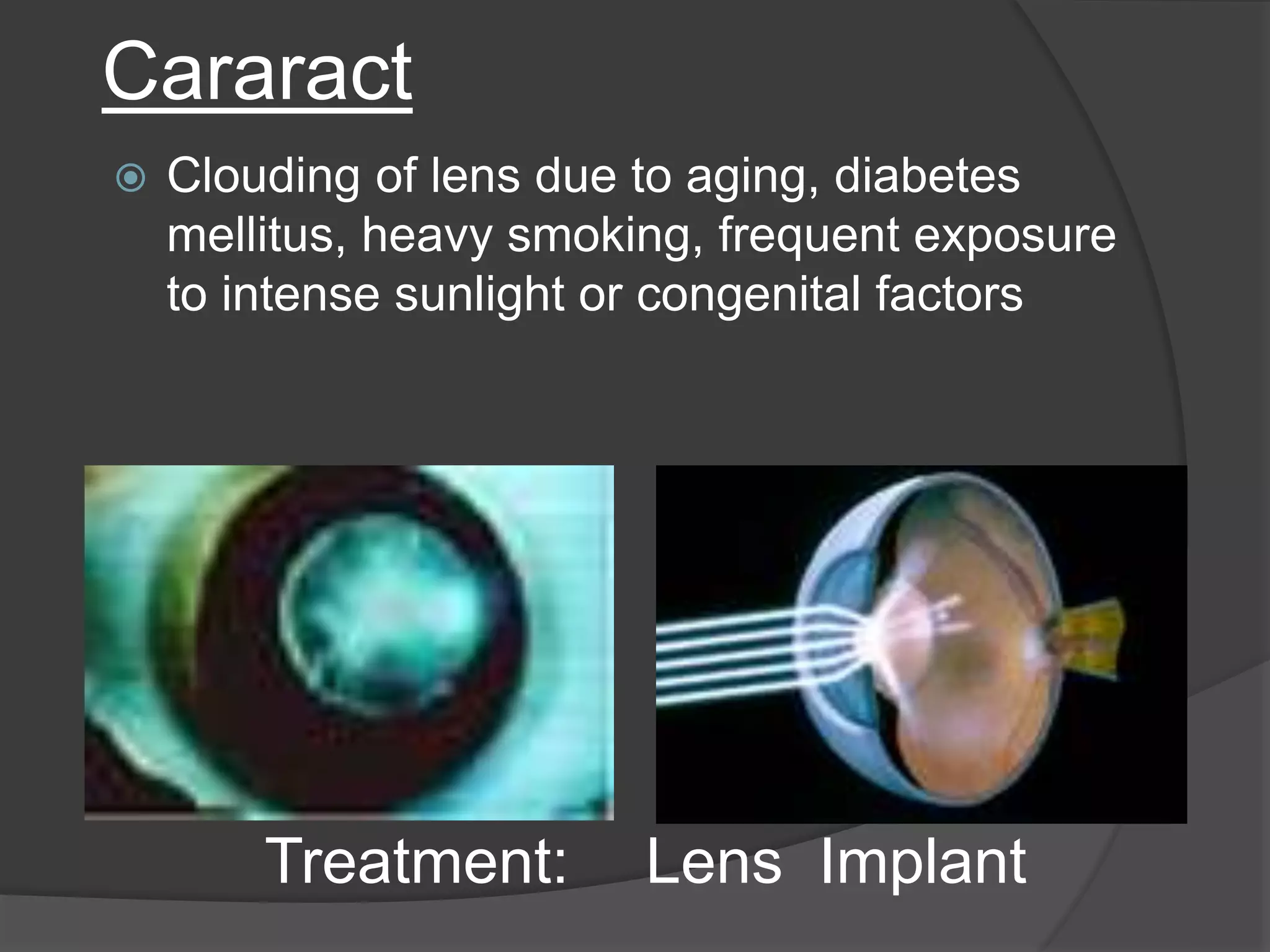
Cataracts involve lens cloudiness due to aging or other factors, with treatment options including lens extraction and replacement.
Visual acuity defines clarity of vision; myopia leads to images focused in front, while hyperopia focuses behind the retina. Astigmatism results in uneven light bending.























































































