Download to read offline
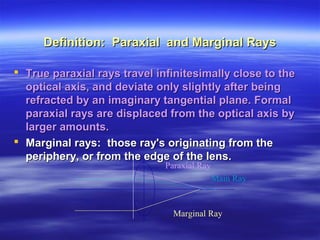







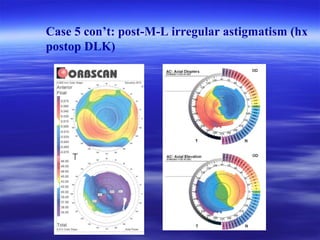
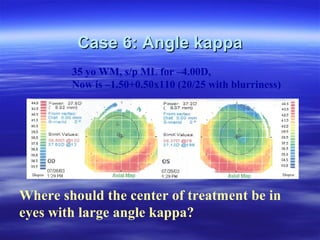


This document discusses paraxial geometrical optics and relevant issues in refractive surgery. It defines key terms like paraxial rays, marginal rays, apertures, pupils, and optical zones. It describes how centering the ablation on the pupil is important to maximize visual function and minimize aberrations. Decentration of more than 0.1-0.2mm can erase benefits of customized ablation. Clinical cases demonstrate problems that can arise from decentration, including glare, halos, and irregular astigmatism. The take-home message is that the ablation center should be centered on the miotic pupil to optimize outcomes.
































![Mafe[1]](https://cdn.slidesharecdn.com/ss_thumbnails/mafe1-110519173429-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)