Downloaded 121 times










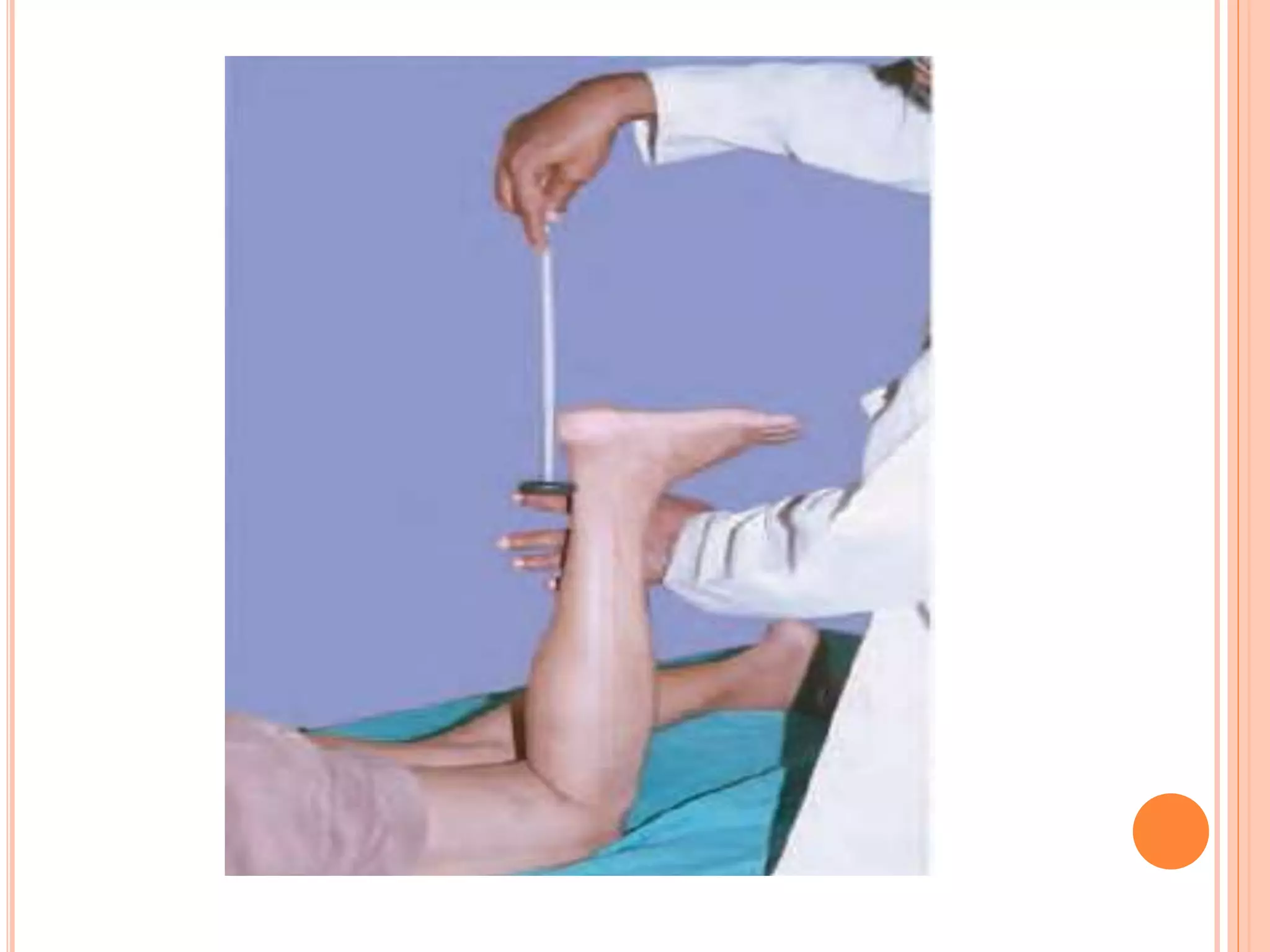
















This document provides an overview of reflexes, including: 1. It defines reflexes as involuntary responses to sensory stimuli and describes the basic reflex arc components. 2. It classifies reflexes based on various criteria and describes how reflexes are graded from absent to exaggerated. 3. It provides instructions for properly eliciting reflexes and lists examples of deep, superficial, and pathological reflexes as well as signs of exaggerated and diminished reflexes.























































































