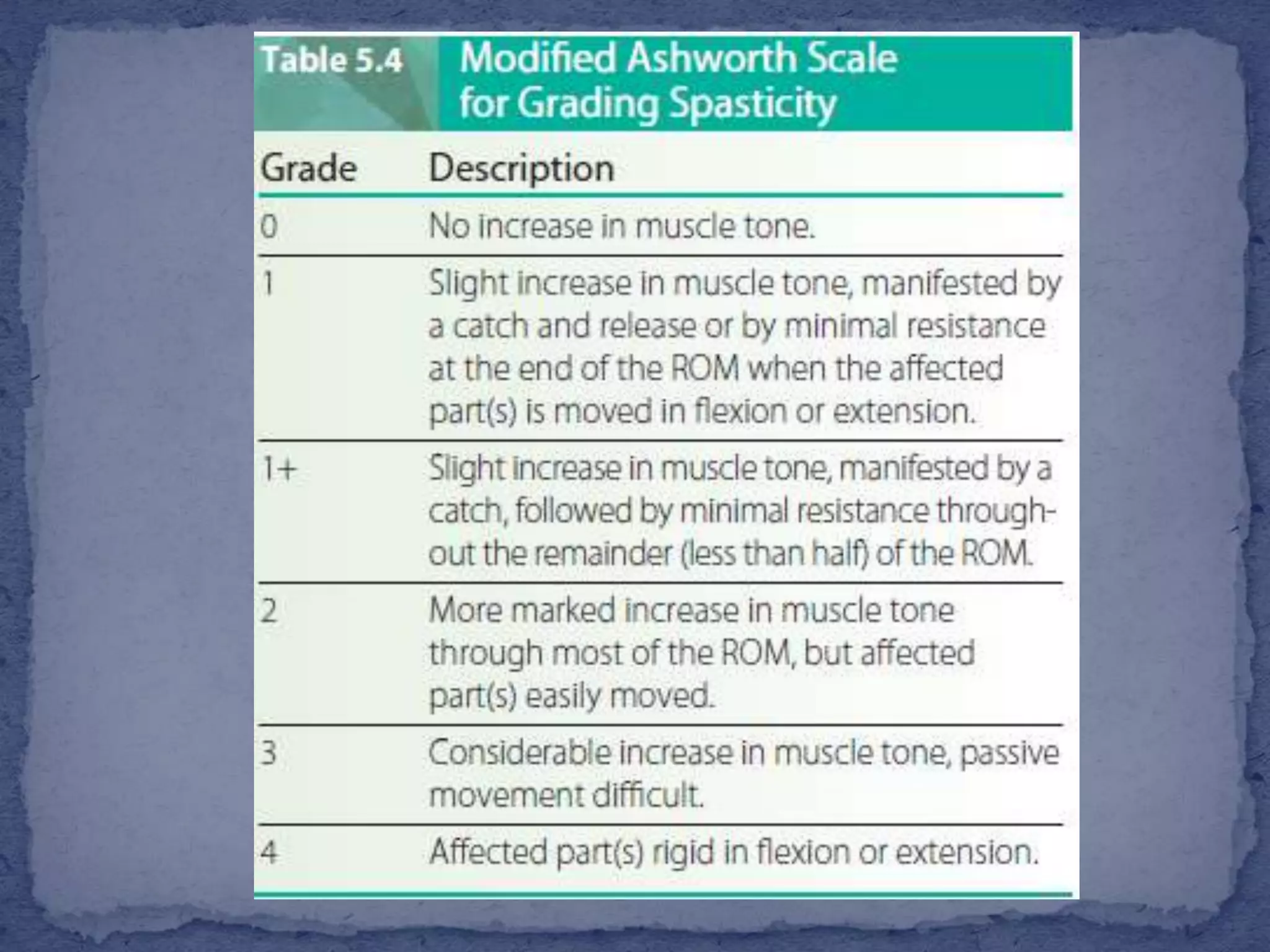
The document discusses various types of muscle tone abnormalities including hypertonia, hypotonia, spasticity, rigidity, dystonia, and their clinical presentations and assessments. Spasticity is characterized by velocity-dependent resistance to stretch and may result in contractures and functional limitations. Rigidity differs from spasticity in being independent of movement velocity. Various assessments of tone are discussed including observation of posture and movement, palpation of muscles, passive range of motion testing, scales like the Modified Ashworth Scale, and reflex testing.







![ Limbs that appear
floppy and lifeless
(e.g., a lower
extremity [LE]
rolled out to the
side in external
rotation) may
indicate
hypotonicity](https://image.slidesharecdn.com/2neuroassessment1469021951611-161128102031/75/Muscle-tone-and-Deep-tendon-reflex-assessment-14-2048.jpg)