Downloaded 124 times
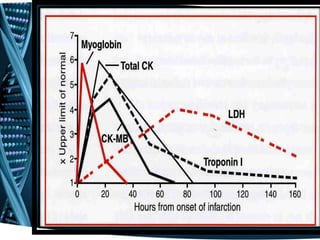
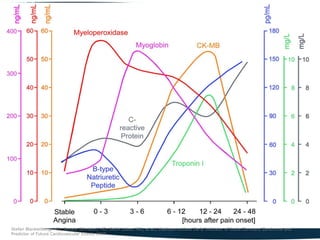
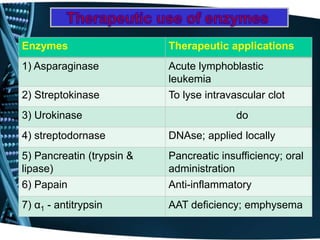


The document discusses the role of serum enzyme measurements in diagnosing various diseases, particularly those related to cardiac and gastrointestinal conditions, highlighting enzyme release as an indicator of cell damage. It details specific enzymes and their time courses in heart diseases, including troponin and BNP as markers for myocardial infarction and heart failure. Additionally, it covers the significance of other enzymes in liver function tests and therapeutic applications, emphasizing that these biochemical markers are crucial for assessing disease presence, severity, and prognosis.


































































![Plasma_Enzymes_of_dental_and_physiotherapy[1].pptx - للقراءة فقط.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/plasmaenzymesofdentalandphysiotherapy1-251003124517-5cb2583b-thumbnail.jpg?width=640&height=640&fit=bounds)

































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






