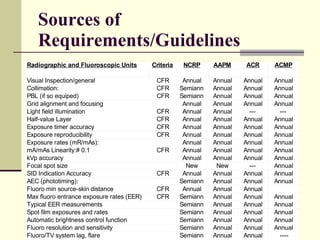
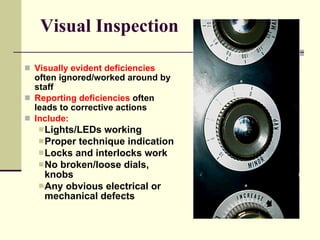
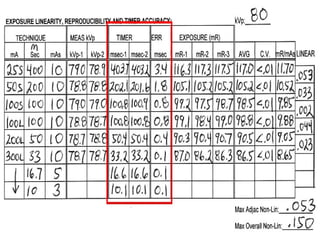
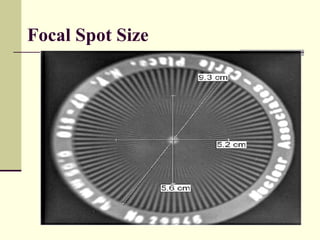
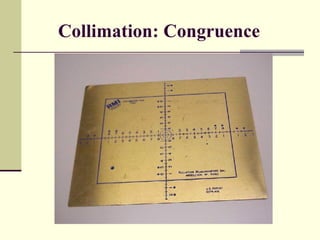
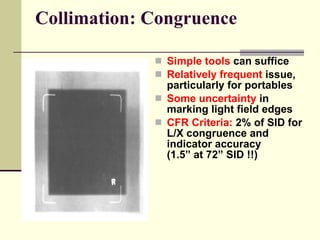
This document discusses quality management and quality control programs for radiographic and fluoroscopic inspections. It describes quality management as encompassing quality assurance and quality improvement to evaluate care using various methodologies. Quality assurance plans and monitors problems to ensure technical requirements are met. Quality control refers to operational techniques used to maintain quality standards throughout the process, from inputs to outputs. The document outlines elements of a typical quality control program, including visual inspections, accuracy testing of kVp, mA, and timers, focal spot testing, and more. It emphasizes the importance of monitoring images and systems to reduce downtime, repeats, dose, and costs while increasing confidence and morale.














![Portable and mobile radiographic equipments [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/portableandmobileradiographicequipmentsautosaved-230729155829-aadaaabd-thumbnail.jpg?width=640&height=640&fit=bounds)


































































