Quality, Quality Control, and Quality Assurance.pptx
1.
Quality, Quality Control,and
Quality Assurance in
Radiographic Services
Ensuring Excellence in Diagnostic
Imaging
Jonathan.C.Shija
2.
Introduction
• Radiographic servicesplay a critical role in
modern healthcare, aiding in accurate
diagnosis and treatment planning.
• Quality in radiography ensures patient safety,
diagnostic reliability, and operational
efficiency.
• Quality Control (QC) and Quality Assurance
(QA) are systematic approaches to maintain
and improve standards.
3.
What is Qualityin Radiography?
Definition:
Quality in radiography refers to the degree of
excellence in diagnostic imaging services, ensuring
that:
• Images are diagnostically accurate (clear, detailed,
and free from artifacts).
• Procedures are safe for patients and staff (following
ALARA—As Low As Reasonably Achievable—
principles).
• Services are efficient, consistent, and patient-
centered.
4.
Key Aspects ofQuality in Radiography
1. Diagnostic Value
1. High-resolution images with optimal contrast, density, and minimal noise.
2. Correct anatomical coverage and positioning (e.g., no missing critical
structures).
2. Radiation Safety
1. Minimal dose exposure while maintaining image quality (ALARA compliance).
2. Proper shielding and collimation to avoid unnecessary radiation.
3. Operational Efficiency
1. Reduced repeat rates (avoiding retakes saves time and reduces patient dose).
2. Proper workflow (e.g., minimal waiting times, organized reporting).
4. Patient & Staff Satisfaction
1. Comfortable experience for patients (clear communication, minimal
discomfort).
2. Ergonomics and safety for radiographers (e.g., reducing occupational radiation
exposure).
5. Regulatory Compliance
1. Meets national/international standards (e.g., AERB, MQSA, ISO, ICRP).
2. Documentation and audit readiness.
5.
Why Does QualityMatter?
• Misdiagnosis risks (e.g., poor-quality images
may miss fractures or tumors).
• Patient harm (excessive radiation, repeated
exposures).
• Legal and financial consequences (non-
compliance with regulations).
6.
Quality Control (QC)in Radiography
Definition:
"QC refers to the set of routine technical procedures that
ensure radiographic equipment, materials, and processes
consistently produce high-quality images with minimal
radiation exposure."
Objectives of QC:
1. Maintain optimal image quality (contrast, resolution,
noise).
2. Detect equipment malfunctions early (e.g., tube leakage,
calibration drift).
3. Minimize patient dose by reducing retakes.
4. Ensure compliance with safety standards (e.g., AERB, ICRP).
Common QC Tools& Devices
• Ionization chambers (for dose
measurements).
• Pinhole cameras (focal spot size evaluation).
• Test objects (e.g., Leeds TOR/CDR for
resolution).
• Densitometers (for film processing
consistency).
9.
Why QC Matters
•Patient Safety: Prevents overexposure due to
equipment errors.
• Cost Savings: Reduces repeat examinations
and wasted resources.
• Regulatory Compliance: Mandatory for
accreditation (e.g., NABH, ISO 9001).
11.
QC Tests &Procedures in Radiography
1. Daily/Weekly QC Checks
• Purpose: Monitor consistency in imaging and processing.
• Visual Inspection:
• Check X-ray tubes, cables, and detectors for damage.
• Ensure cleanliness of cassettes/DR detectors.
• Darkroom (if using film):
• Clean processor rollers.
• Check chemical levels and temperature.
• Laser Printer (if applicable):
• Verify uniformity and artifact-free prints.
12.
2. Equipment CalibrationTests
• Purpose: Ensure accurate exposure parameters.
• kVp and mA Accuracy:
• Use a kVp meter to verify output vs. selected settings.
• Measure mA linearity across different settings.
• Timer Accuracy:
• Test short exposure times (e.g., 0.01s–0.1s) with a
spinning top test.
• Beam Alignment & Collimation:
• Light field vs. radiation field alignment (should match
within ±2% of SID).
• Collimator centering test (using a star pattern tool).
13.
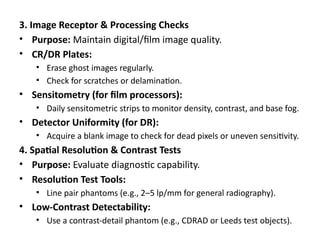
3. Image Receptor& Processing Checks
• Purpose: Maintain digital/film image quality.
• CR/DR Plates:
• Erase ghost images regularly.
• Check for scratches or delamination.
• Sensitometry (for film processors):
• Daily sensitometric strips to monitor density, contrast, and base fog.
• Detector Uniformity (for DR):
• Acquire a blank image to check for dead pixels or uneven sensitivity.
4. Spatial Resolution & Contrast Tests
• Purpose: Evaluate diagnostic capability.
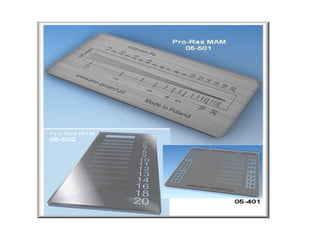
• Resolution Test Tools:
• Line pair phantoms (e.g., 2–5 lp/mm for general radiography).
• Low-Contrast Detectability:
• Use a contrast-detail phantom (e.g., CDRAD or Leeds test objects).
14.
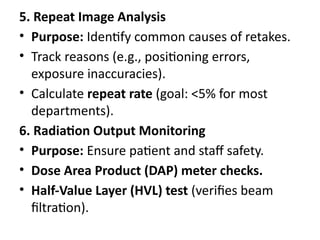
5. Repeat ImageAnalysis
• Purpose: Identify common causes of retakes.
• Track reasons (e.g., positioning errors,
exposure inaccuracies).
• Calculate repeat rate (goal: <5% for most
departments).
6. Radiation Output Monitoring
• Purpose: Ensure patient and staff safety.
• Dose Area Product (DAP) meter checks.
• Half-Value Layer (HVL) test (verifies beam
filtration).
16.
Quality Assurance (QA)in Radiography
1. Definition of QA:
• "A systematic approach to ensure consistent,
high-quality diagnostic imaging while
minimizing risks to patients and staff."
• Key Goal: Prevent errors rather than detect
them (proactive vs. reactive).
17.
2. Scope ofQA in Radiography:
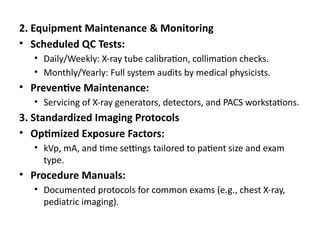
• Equipment: Regular maintenance, calibration,
and performance checks.
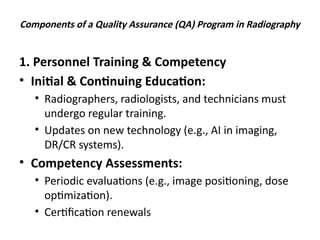
• Personnel: Training, competency assessments,
and continuing education.
• Processes: Standardized protocols for imaging,
reporting, and patient handling.
• Outcomes: Monitoring diagnostic accuracy,
repeat rates, and patient dose audits.
18.
3. Components ofa QA Program:
1.Policies & Procedures:
1.Documented protocols for each exam type (e.g., chest X-
ray, mammography).
2.Equipment Management:
1.Scheduled QC tests (e.g., kVp accuracy, beam alignment).
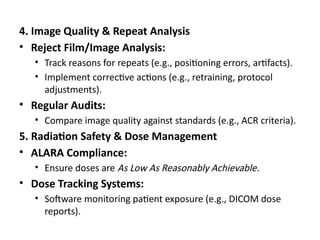
3.Patient Dose Optimization:
1.Follow ALARA (As Low As Reasonably Achievable)
principles.
4.Audits & Feedback:
1.Review repeat rates, radiologist reports, and patient
complaints.
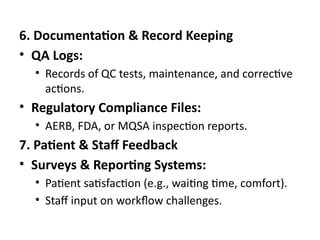
6. Documentation &Record Keeping
• QA Logs:
• Records of QC tests, maintenance, and corrective
actions.
• Regulatory Compliance Files:
• AERB, FDA, or MQSA inspection reports.
7. Patient & Staff Feedback
• Surveys & Reporting Systems:
• Patient satisfaction (e.g., waiting time, comfort).
• Staff input on workflow challenges.
26.
8. Continuous Improvement
•Regular QA Meetings:
• Review incidents, updates, and new best practices.
• Benchmarking:
• Compare performance with other departments or
national standards.
27.
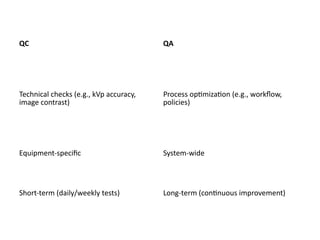
Differences Between QCand QA
1. Definition
• QC: Reactive process focused on detecting
defects in equipment, images, or procedures.
• Example: Checking X-ray machine calibration or
image artifacts.
• QA: Proactive process focused on preventing
defects through systemic improvements.
• Example: Implementing standardized protocols or
staff training programs.
4. Goal
• QC:Ensure consistency in equipment and
image quality.
• QA: Ensure overall excellence in radiographic
services.
31.
Importance of QA/QCin Radiography
1. Ensures Patient Safety
• Minimizes Radiation Exposure:
• QC checks ensure equipment delivers the correct dose
(ALARA principle: As Low As Reasonably Achievable).
• Prevents overexposure due to faulty machines or
incorrect settings.
• Reduces Errors:
• QA programs standardize protocols to avoid mistakes
(e.g., wrong patient, incorrect positioning).
32.
2. Enhances DiagnosticAccuracy
• High-Quality Images:
• QC maintains optimal image clarity, contrast, and resolution.
• Reduces artifacts (e.g., fogging, scratches) that could mislead
diagnoses.
• Fewer Retakes:
• Proper QA/QC minimizes repeat exposures, saving time and
reducing patient dose.
3. Regulatory & Legal Compliance
• Meets Standards:
• Required by regulatory bodies (e.g., AERB, MQSA, ICRP, ISO).
• Avoids legal penalties or facility shutdowns.
• Documentation & Audits:
• QA ensures records are maintained for inspections.
33.
4. Cost Efficiency
•Prevents Equipment Downtime:
• Regular QC detects issues early (e.g., tube failures, calibration
drift).
• Reduces Waste:
• Fewer repeat exams save film/digital storage and processing
costs.
5. Improves Workflow & Staff Confidence
• Standardized Protocols (QA):
• Clear guidelines improve efficiency and reduce variability
between technologists.
• Staff Training & Competency:
• QA programs ensure continuous education, boosting
confidence in handling complex cases.
34.
6. Enhances PatientTrust & Satisfaction
• Faster, Safer Exams:
• Patients experience fewer delays and retakes.
• Professional Reputation:
• Consistent quality builds trust in healthcare
providers.
35.
Barriers to EffectiveQuality Management in
Radiology
1. Financial Constraints
• High Costs:
• Regular equipment calibration and maintenance.
• Upgrading outdated systems (e.g., analog to digital).
• Training programs for staff.
• Budget Limitations:
• Small clinics may prioritize immediate needs over long-term QA
investments.
2. Staff Resistance & Training Gaps
• Lack of Awareness:
• Technologists may view QA as an extra burden.
• Insufficient Training:
• New protocols require continuous education.
• Workload Pressure:
• QA tasks may be neglected during high patient turnover.
36.
3. Technological Advancements
•Keeping Up with Changes:
• Rapid evolution of imaging tech (AI, DR, PACS)
demands frequent updates to QA protocols.
• Compatibility Issues:
• Integrating new software/hardware with existing
systems.
4. Regulatory & Compliance Hurdles
• Complex Standards:
• Adhering to AERB, MQSA, ISO, or JCI requirements.
• Documentation Burden:
• Maintaining logs for audits can be time-consuming.
37.
5. Cultural &Organizational Barriers
• Lack of Leadership Support:
• Management may not prioritize QA without immediate
ROI.
• Inconsistent Practices:
• Variability between departments or shifts.
6. Patient-Related Factors
• Non-Compliance:
• Patients may move during exams, affecting image quality.
• High Demand:
• Pressure to shorten exam times can compromise QC
checks.
38.
Overcoming QA/QC Challenges
Solutions:
•Cost Management:
• Prioritize critical QC tests (e.g., monthly kVp checks).
• Seek grants or government subsidies for upgrades.
• Staff Engagement:
• Workshops to demonstrate QA’s impact on workflow
efficiency.
• Incentivize compliance (e.g., recognition programs).
• Technology Integration:
• Use automated QC tools (e.g., AI for image analysis).
• Standardization:
• Create clear, department-wide SOPs aligned with regulations.
39.
Case Study –Reducing Repeat Rates Through QA/QC
Background:
• Hospital: XYZ Medical Center (300-bed facility)
• Issue: High repeat/rejection rates (15%) in
general radiography, leading to:
• Increased patient radiation exposure.
• Delays in diagnosis.
• Higher operational costs.
40.
QA/QC Interventions:
1.Equipment Calibration:
1.Regularchecks of kVp, mA, and timer accuracy (monthly QC).
2.Found +10% deviation in kVp in one X-ray tube →
recalibrated.
2.Technician Training:
1.Workshops on optimal positioning techniques (e.g., reducing
motion artifacts).
2.Standardized exposure protocols for common exams (e.g.,
chest X-rays).
3.Image Review Audits:
1.Weekly random audits of rejected images to identify
recurring issues (e.g., collimation errors).
41.
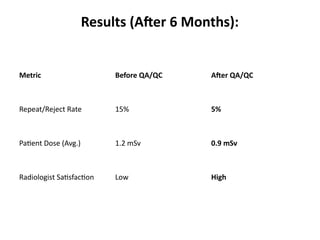
Results (After 6Months):
Metric Before QA/QC After QA/QC
Repeat/Reject Rate 15% 5%
Patient Dose (Avg.) 1.2 mSv 0.9 mSv
Radiologist Satisfaction Low High
42.
Key Takeaways:
• ProactiveQA/QC reduced operational costs
and improved patient safety.
• Continuous monitoring is essential to sustain
results.
43.
Conclusion
Key Takeaways:
1. Qualityin Radiography ensures diagnostic accuracy,
patient safety, and operational efficiency.
2. Quality Control (QC) focuses on technical checks
(equipment calibration, image quality tests) to maintain
consistency.
3. Quality Assurance (QA) is a systematic approach
(policies, training, audits) to improve overall service
standards.
4. QA & QC together reduce repeat rates, minimize
radiation exposure, and enhance compliance with
regulatory bodies (
44.
• Final Thought:
"Qualityis never an accident; it is always the
result of intelligent effort." – John Ruskin
• Continuous improvement in radiographic
services requires commitment from all
stakeholders (technologists, radiologists,
administrators).
• Investing in QA/QC leads to better patient
outcomes and long-term cost savings.
45.
THANK YOU
"Quality isnever an accident; it is always the result of
intelligent effort." – John Ruskin