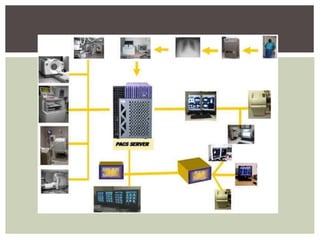
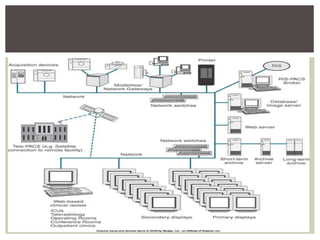
PACS (Picture Archiving and Communications System) is a medical imaging technology that provides economical storage and access to images from multiple modalities. It began development in the 1950s and was further advanced by the military in the 1980s. PACS replaces film storage with electronic images that can be accessed from various workstations and remotely. It consists of imaging modalities, a network, workstations, and archives. PACS provides benefits like hard copy replacement, remote access, and integration with other medical systems, but high costs and need for training were initial disadvantages.






































![Picture Archival and Communication System [PACS] - Overview](https://cdn.slidesharecdn.com/ss_thumbnails/picturearchivalandcommunicationsystem-overview-140111015852-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

































































