Downloaded 621 times

![Investigations
Non invasive : USG abdomen, USG neck for lymph node, CT scan of
chest and abdomen or other specific areas, 2D echo (two dimensional
echocardiography), trans-esophageal echo, infectious disease serology
like brucella, rickettsia, ANA (antinuclear antibodies) ds-DNA (double
stranded deoxyribo nucleic acid), C-ANCA, P-ANCA (P - Antineutrophilic
cytoplasmic antibodies), C3 (complement 3), C4 (complement 4) levels,
ACE (angiotensin converting enzyme) levels, ferritin, thyroid function
tests and tumor markers [like PSA (prostate specific antigen), CEA
(carcino embryonic antigen)].
Specific investigations](https://image.slidesharecdn.com/pyrexiaofunknownorigin-151102111339-lva1-app6892/75/Pyrexia-of-unknown-origin-22-2048.jpg)


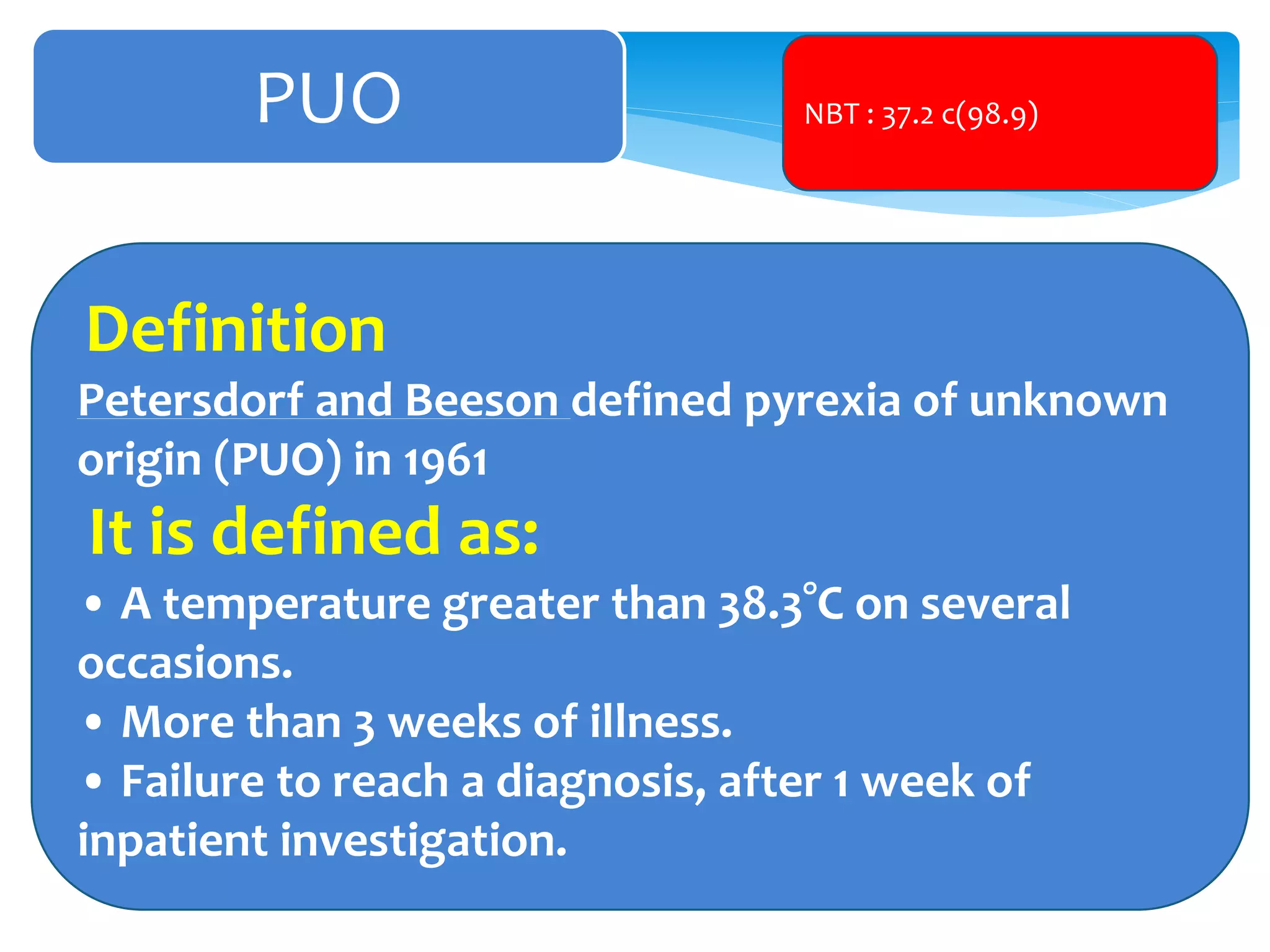
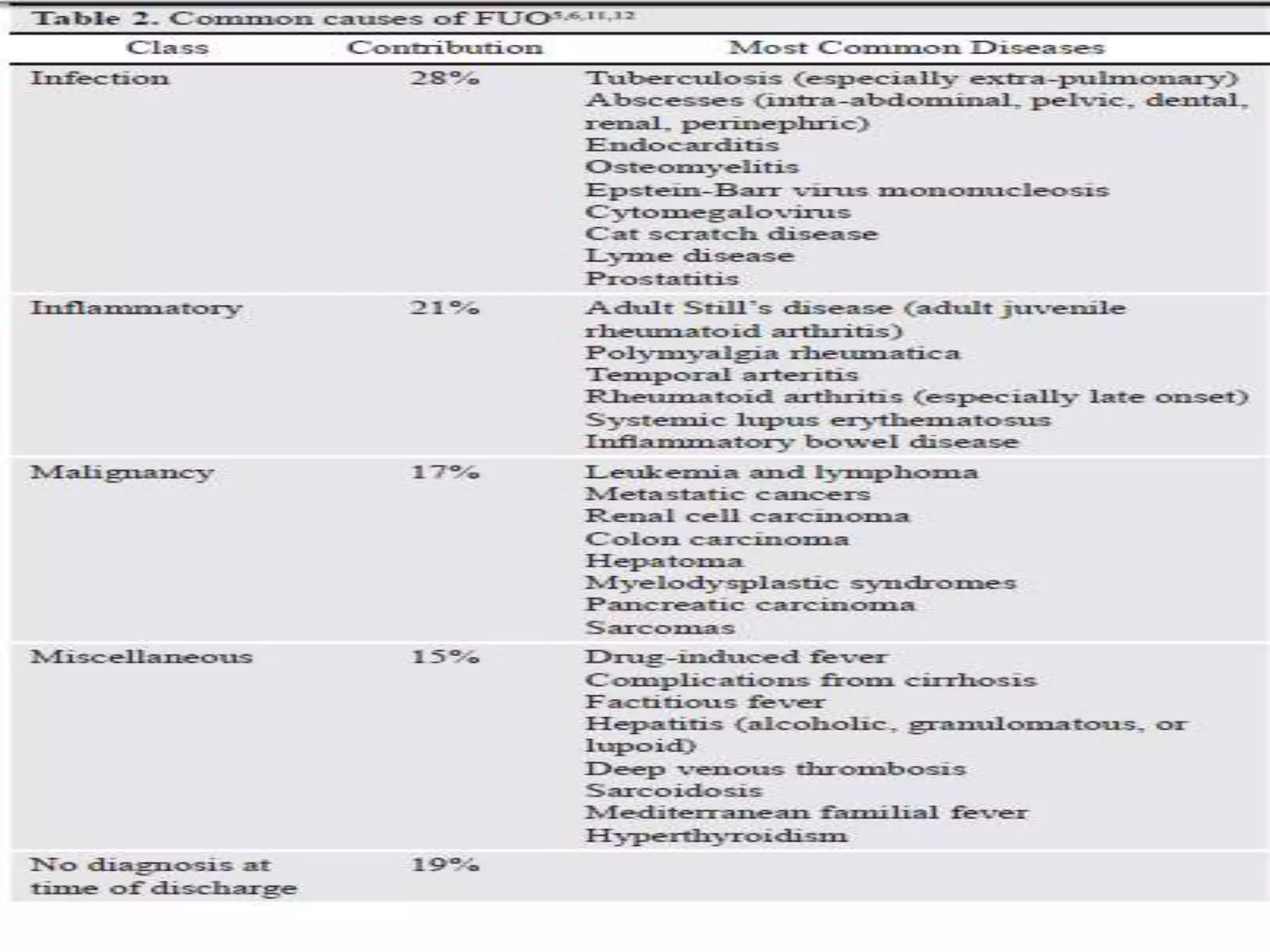
Pyrexia of Unknown Origin (PUO) is defined as a fever over 38.3°C on multiple occasions for more than 3 weeks without a diagnosis after a week of inpatient investigations. Common causes include infections like tuberculosis, abscesses, or endocarditis, inflammatory conditions such as adult Still's disease or systemic lupus erythematosus, and malignancies. A thorough history, physical exam, and baseline investigations are crucial, along with repeating tests and considering more invasive procedures if needed. The diagnostic approach involves 4 stages: collecting a detailed history, comprehensive exam, initial non-invasive investigations, and potentially empirical therapy or therapeutic trials if the cause remains unknown.
Introduces PUO, its significance in medicine, and highlights the historical impact of fever on mortality.
Defines PUO based on criteria by Petersdorf and Beeson, providing temperature and illness duration thresholds.
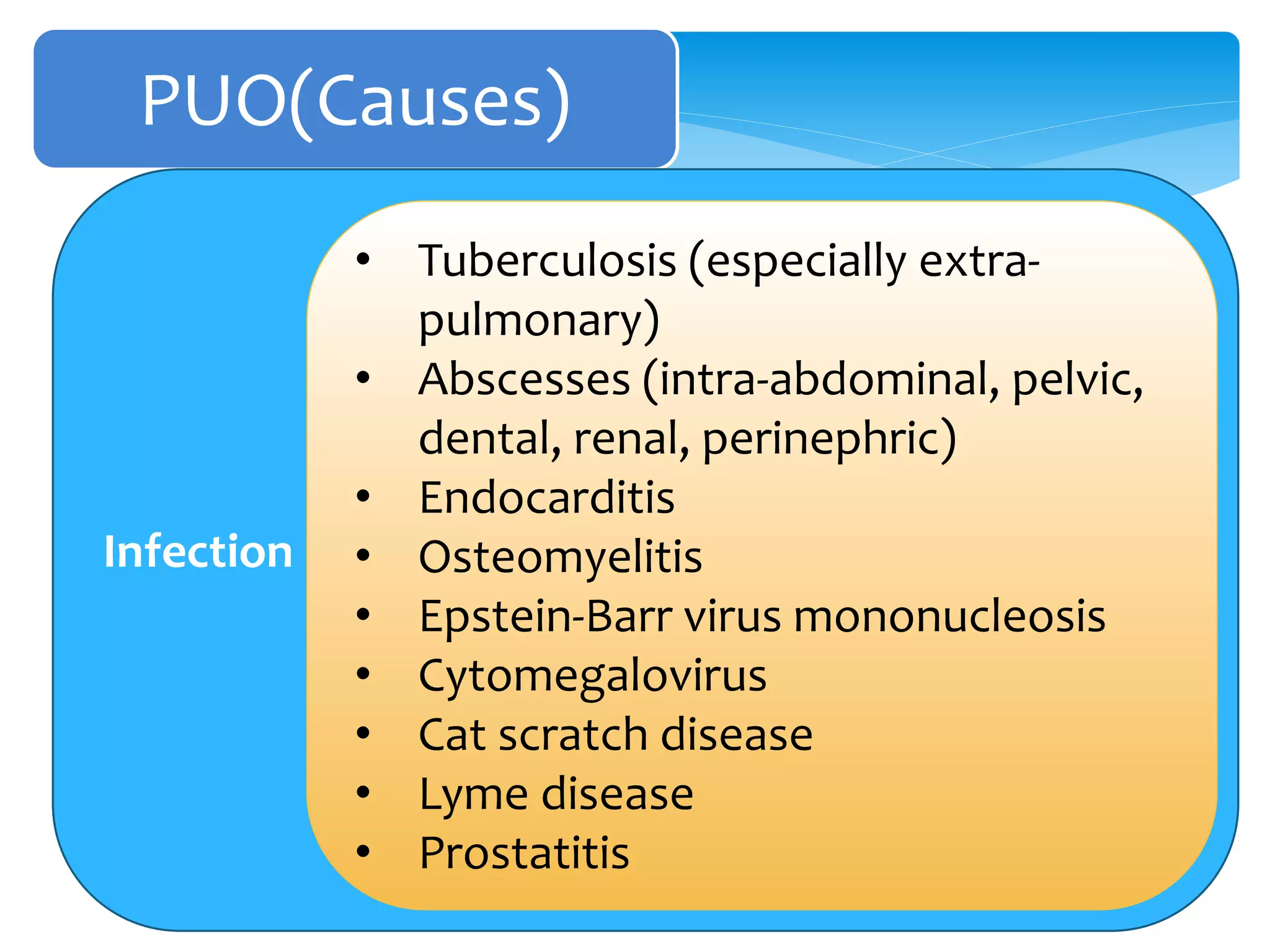
Lists infectious causes including tuberculosis, abscesses, endocarditis, and viral infections.
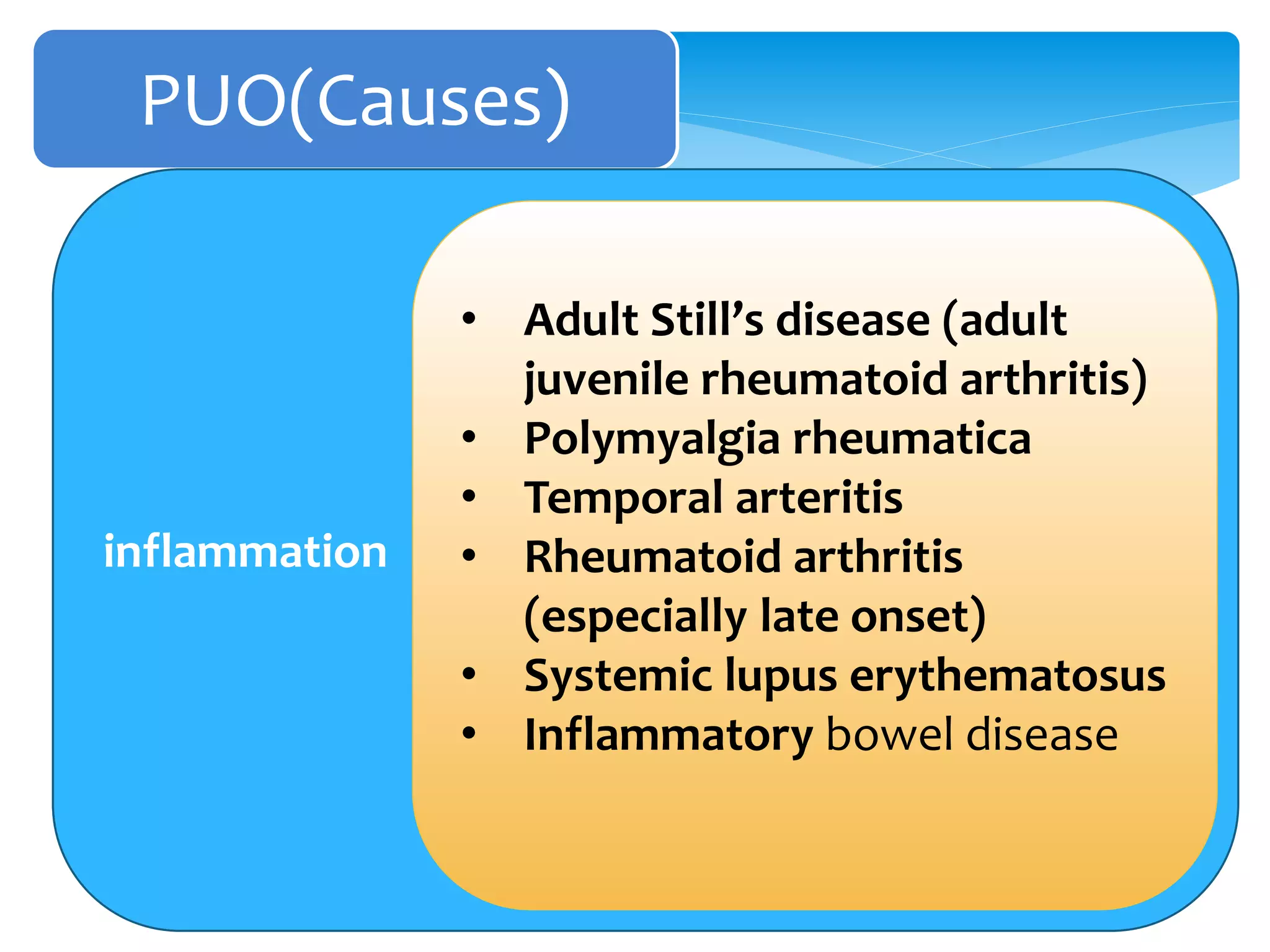
Discusses inflammatory causes such as Adult Still’s disease, rheumatoid arthritis, and systemic lupus.
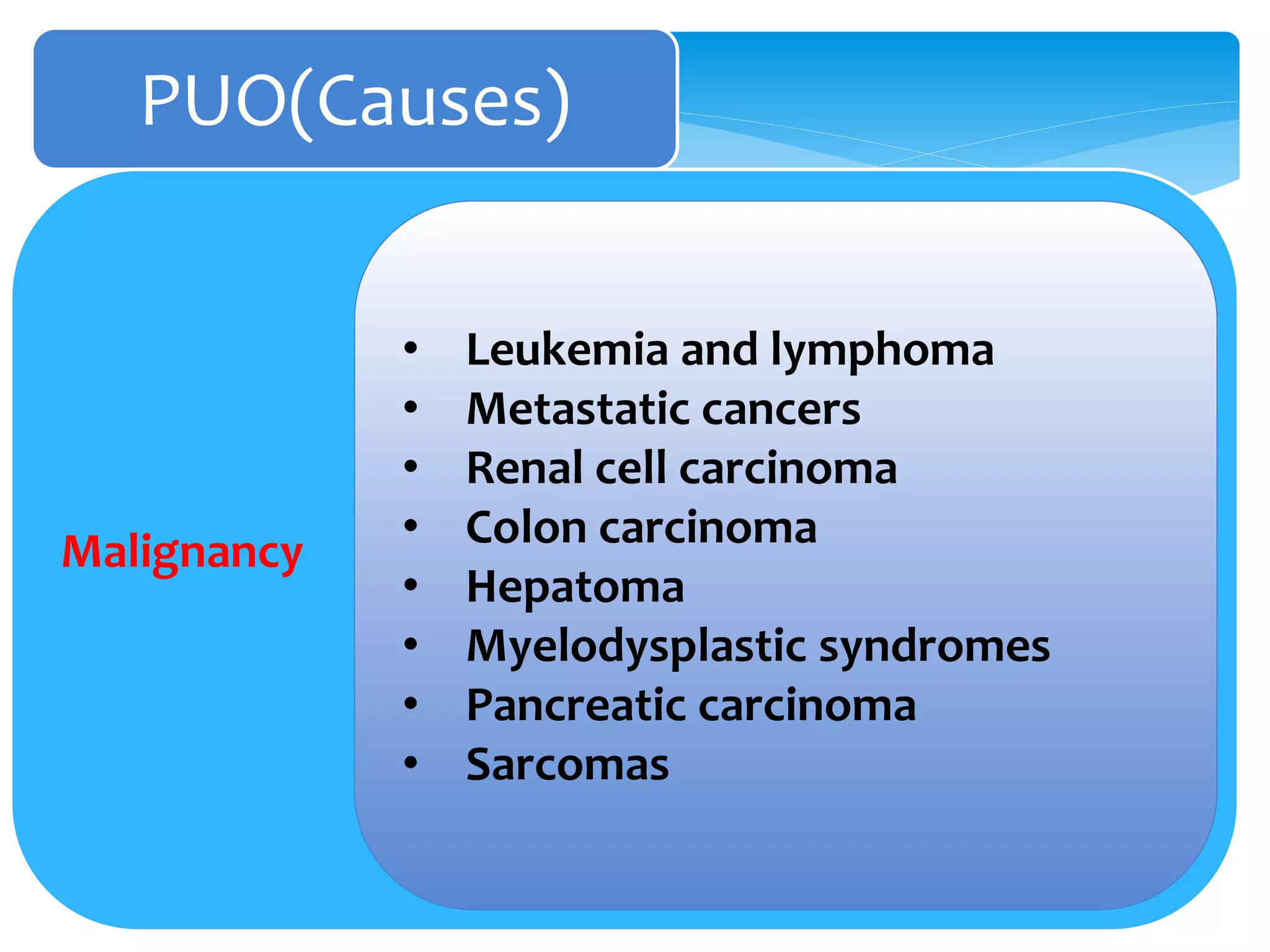
Mentions various malignancies like leukemia, lymphoma, and metastatic cancers contributing to PUO.
Identifies miscellaneous causes including drug-induced fever and complications from liver diseases.
Emphasizes the importance of confirming fever and methodical assessment through history and examination.
Outlines essential points for obtaining a thorough patient history related to fever, symptoms, and risk factors.
Describes the necessity of a comprehensive physical examination to document fever and rule out factitious causes.
Details baseline and specific investigations, including both non-invasive and invasive tests for diagnosis.
Describes conditions under which empirical therapy is advised when a cause for fever isn't identified promptly.
Summarizes the discussion on PUO and closes the presentation.









































































