Downloaded 17 times

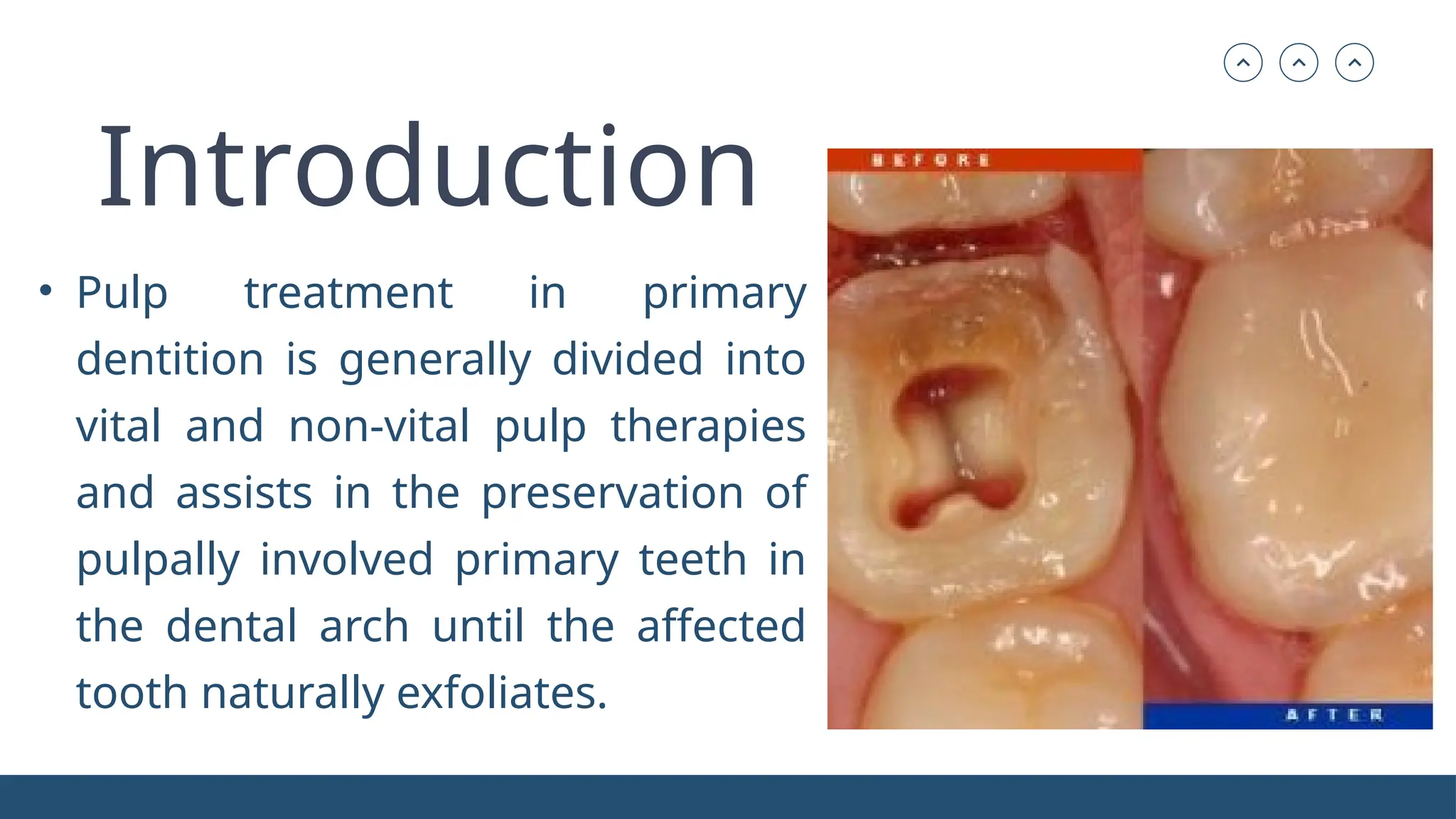





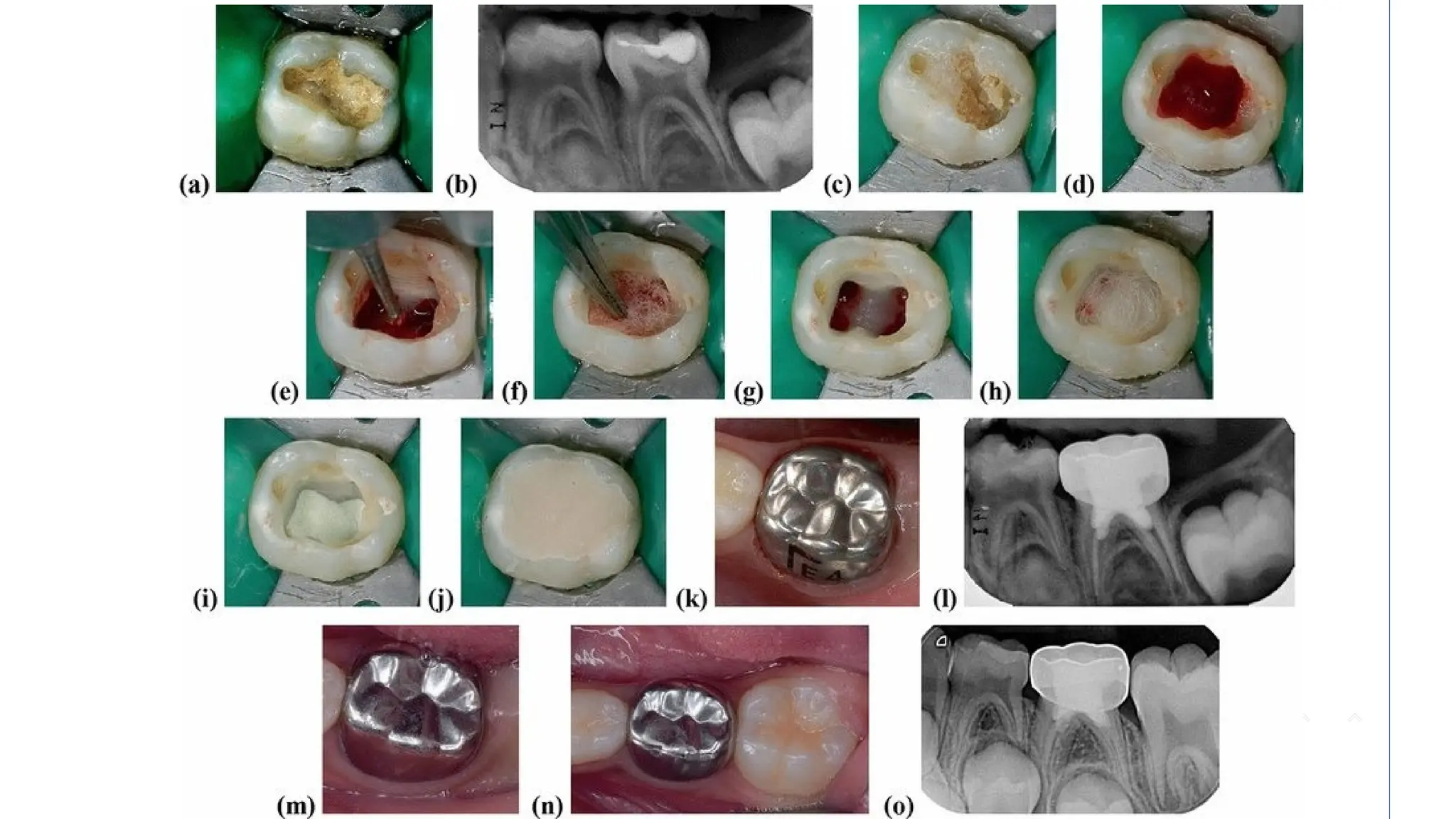





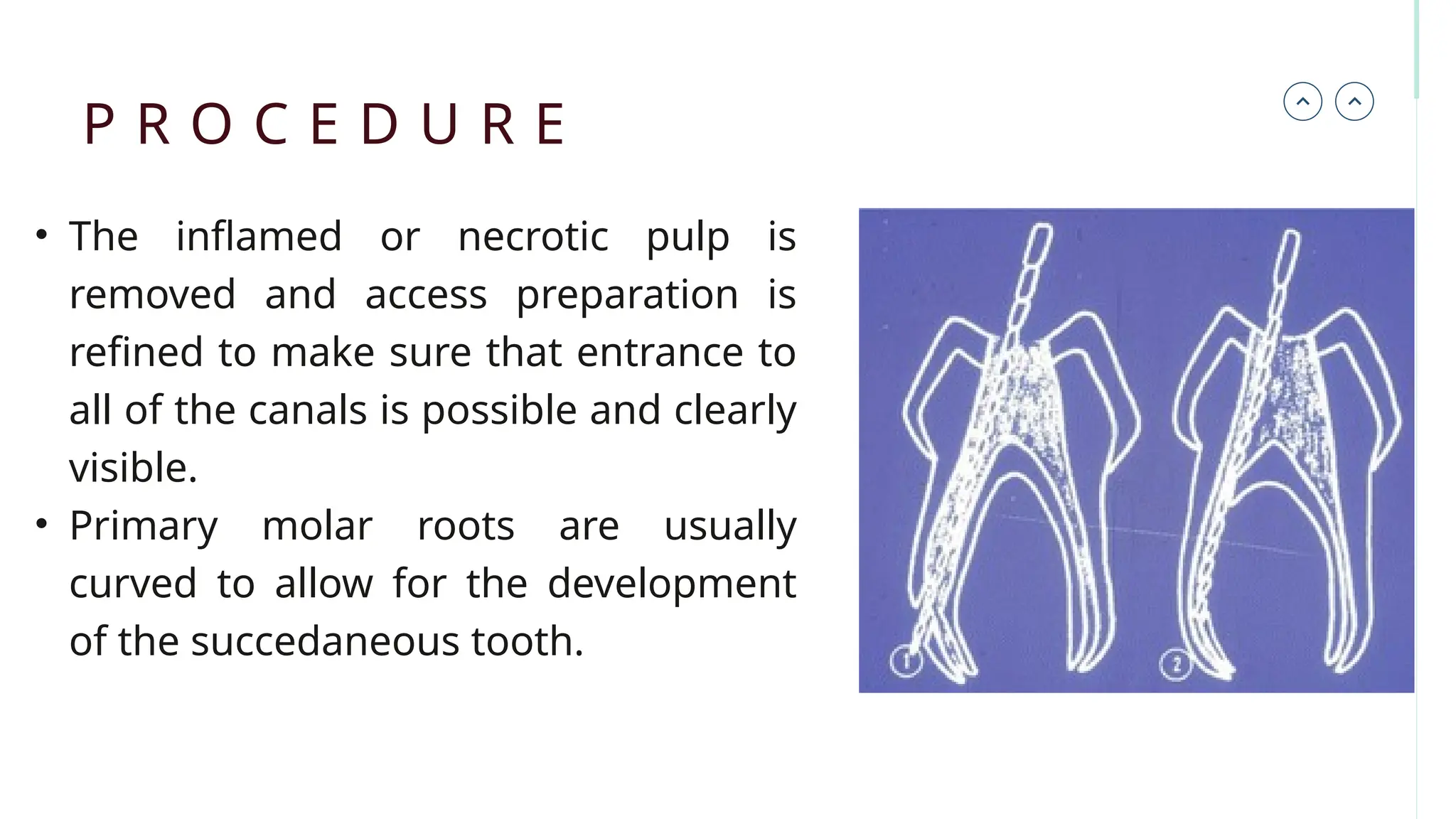




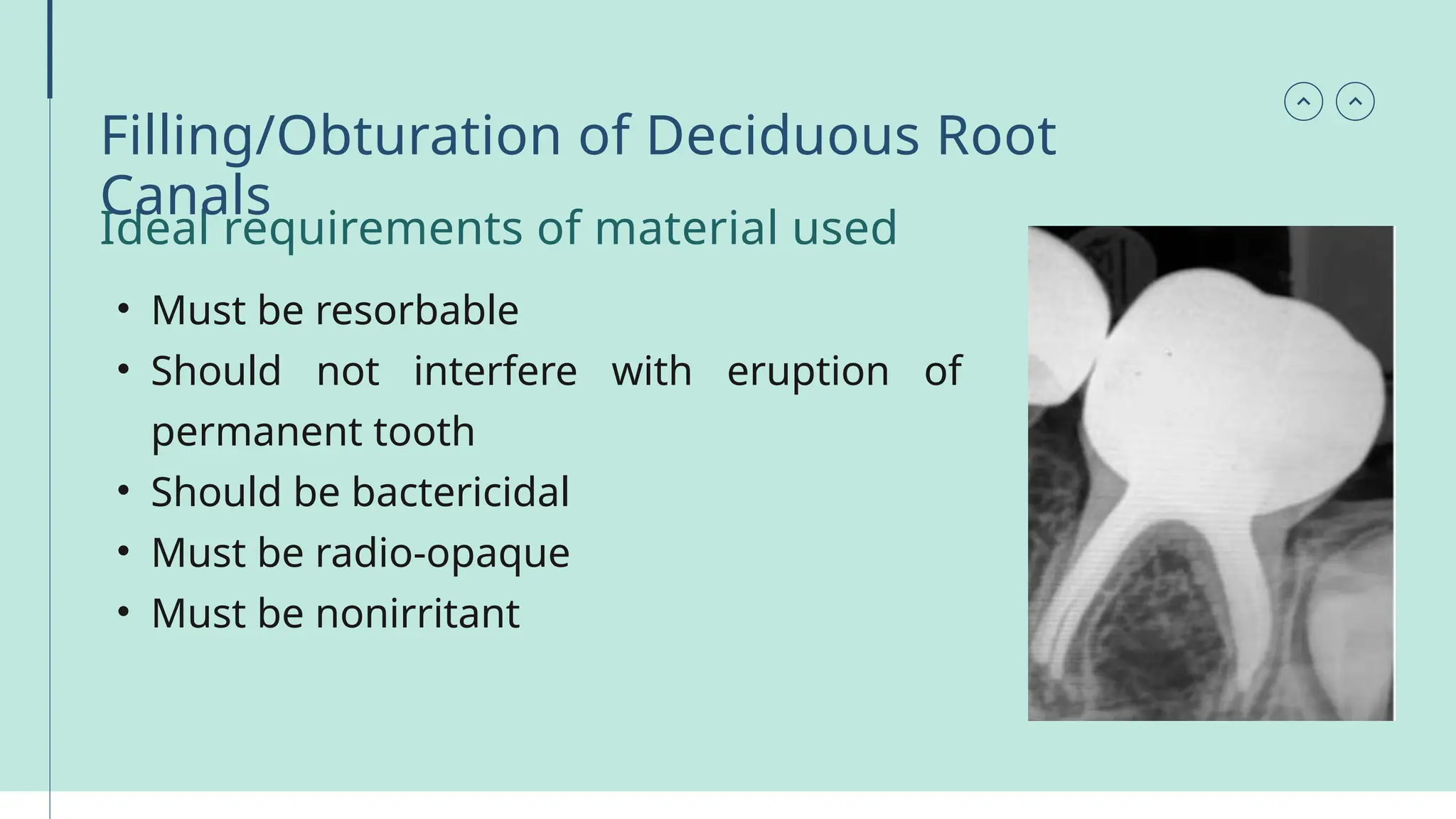


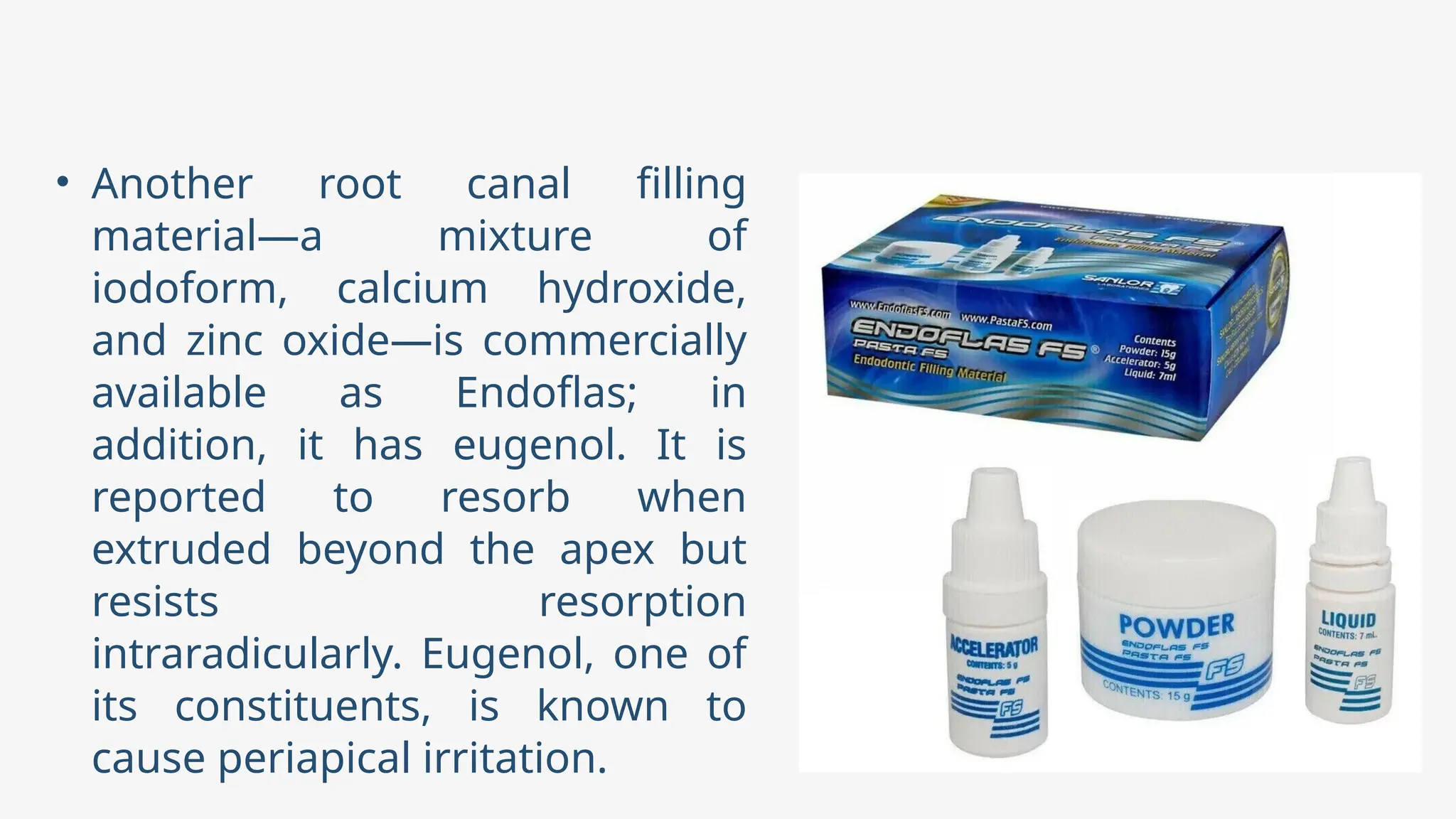












Pulp therapy in primary teeth includes vital and non-vital methods aimed at preserving affected teeth until natural exfoliation. The document details procedures such as pulpotomy and pulpectomy, indicating specific contraindications and preferred materials for each method. It emphasizes the importance of clinical evaluation and successful treatment outcomes in managing pulpally involved primary dentition.















































































