Additional reasons topreserve the integrity of
the primary dentition are to
1. Reduce the likelihood of tooth drift and the resultant malocclusion.
2. Aid in mastication.
3. Preserve a pulpally involved primary tooth in the absence of a succedaneous
tooth.
4. Prevent possible speech problems.
5. Maintain esthetics.
6. Maintain normal eruption time of the succedaneous teeth.
7. Prevent the psychological effects associated with early tooth loss.
Pulpotomy
Pulpotomy is definedas “Surgical removal of the entire
coronal pulp, leaving intact the vital tissue in the canals,
followed by placement of a suitable medicament or
dressing over the remaining pulp stump in an attempt
to promote healing and retention of this vital tissue”.
6.
Indication for pulpotomy
1)Carious or mechanical exposure of vital primary
teeth and young permanent teeth, where
inflammation is restricted to coronal pulp only.
2) Hemorrhage from exposure sites bright red
and be controlled.
3) Absence of abscess or fistula.
4) No interradicular bone loss.
7.
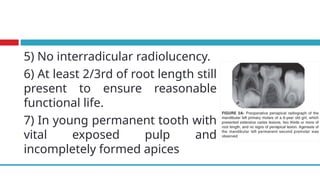
5) No interradicularradiolucency.
6) At least 2/3rd of root length still
present to ensure reasonable
functional life.
7) In young permanent tooth with
vital exposed pulp and
incompletely formed apices
8.
Contraindication of pulpotomy
1.History of spontaneous pain.
2. Swelling
3. Fistula
4. Tenderness to percussion
5. Pathological mobility
6. External/internal root resorption
7. Periapical or interradicular radiolucency
9.
8- Pulp calcifications
9-Pus or exudate from exposures site
10- Uncontrolled bleeding from the amputated pulp
stump
11- Root resorption more than 1/3rd of root length
Devitalizing
◻These products aredesigned to mummify the
remaining pulp tissue and are represented by
formocresol, laser, and electro surgery.
◻As the most universally accepted method,
formocresol will be discussed
◻Formacresol: Buckley’s formula or 20%
formacresol is used
12.
▪ Anesthetize thetooth and isolate with rubber dam.
↓
▪ All caries should be removed.
↓
▪ Entire roof of the pulp chamber is cut with high speed bur and
water spray.
↓
▪ The coronal pulp is removed with the round bur or spoon
excavator.
↓
▪ Pulp chamber is washed thoroughly with saline, to remove all
debris.
↓
Technique for Pulpotomy of the Primary Teeth
13.
▪ Pulp statusis assessed.
↓
▪ Cotton pellet moistened with 1/5th
dilution formacresol is placed
over the amputated pulp for 5 min.
↓
▪ When the cotton pellet is removed, the pulp stump must appear
dark brown or even black, as a result of fixation.
↓
▪ Place ZOE cement in the pulp chamber
↓
▪ Recall after one week and restore with a permanent restoration
if patient is asymptomatic
↓
▪ Place a stainless steel crown
14.
Tooth isolated witha
rubber dam prior to caries
removal
Pulp exposed prior to de-
roofing the pulp chamber
Root canal orifices
showing vital tissue after
Preserving
◻The objective ofthe materials included in this
category is to minimally insult the tissue in order
to preserve the vitality of the radicular pulp.
◻As representatives of this category:
- glutaraldehyde
- ferric sulfate
- sodium hypochlorite (NaOCl)
17.
Glutaraldehyde
⮚ It hasbeen widely tested, to replace
formacresol. Studies have shown that
application of 2-4% produces rapid surface
fixation of the underlying pulp tissue.
⮚ Excellent antimicrobial property
⮚ 15-20 times less toxic than formacresol
18.
Glutaraldehyde Pulpotomy Technique
⮚The glutaraldehyde pulpotomy technique is identical
to the formocresol pulpotomy technique with the
exception that the solution on the cotton pellet is not
expressed.
⮚ Studies have shown variation in success based on
the relative wetness of the cotton pellet .
⮚ The recommendation currently is to have the cotton
pellet soaked in glutaraldehyde and applied very wet.
19.
Ferric Sulfate PulpotomyTechnique
1. Once the pulp chamber is accessed, the coronal pulp
is removed and gross hemostasis is achieved with a
cotton pellet.
2. A 15.5 % ferric sulfate solution is applied to burnish
the pulp stumps for 15 seconds, rinsed away and
dried with cotton pellet. Notice the typical dark
appearance of the tissue affected by the ferric
sulfate.
3. A thick paste of ZOE or IRM is placed in the chamber
20.
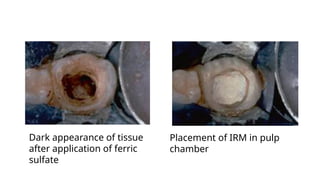
Dark appearance oftissue
after application of ferric
sulfate
Placement of IRM in pulp
chamber
21.
Sodium Hypochlorite PulpotomyTechnique
1. Once the pulp chamber is accessed, the coronal pulp is
removed and hemostasis is achieved with a cotton pellet.
2. A cotton pellet is moistened in 3 % or 5 % NaOCl and
placed in the chamber for 30 s.
3. The pellet is removed, the chamber is gently irrigated
ensuring no clot is present.
4. ZOE is placed in the pulp chamber and the tooth is
restored
22.
Regenerating
⮚ Materials thatbelong to this category of pulpotomy
medicaments can induce reparative dentin, and their
application has been based on sound biologic principles.
⮚ Representatives of this category are calcium hydroxide
(CaOH2) and mineral trioxide aggregate (MTA).
Pulpectomy
◻Pulpectomy is definedas “Removal of the
entire pulp and subsequent filling of the
canals of the primary teeth with a suitable
resorbable material”.
25.
Indications for pulpectomy
1.Primary teeth with pulp inflammation
extending beyond the coronal pulp
2. Roots and alveolar bone with minimum
pathologic
3. Primary teeth with necrotic pulp and or
periapical abscess
4. Pus at the clinical pulp exposure site
26.
Contraindication
1. Grossly destroyedtooth that is non restorable
clinically
2. Periradicular involvement extending to the
permanent tooth bud, where the risk of
damage to the permanent tooth is high.
3. Root resorption - internal or external
4. Extensive mobility
5. Gross bone loss at the apex or at the furcation
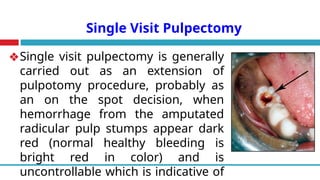
Single Visit Pulpectomy
❖Singlevisit pulpectomy is generally
carried out as an extension of
pulpotomy procedure, probably as
an on the spot decision, when
hemorrhage from the amputated
radicular pulp stumps appear dark
red (normal healthy bleeding is
bright red in color) and is
uncontrollable which is indicative of
29.
◻Other indication ofsingle visit pulpectomy is a
tooth with history of spontaneous pain without
pulp necrosis, abscess or a fistula.
30.
Procedure of singlevisit pulpectomy
1. Done under local anesthesia and rubber dam isolation
2. All caries should be removed.
3. Entire roof of the pulp chamber is cut with high speed
bur and water spray.
4. The coronal pulp is removed with the round bur or spoon
excavator.
5. Pulp chamber is washed thoroughly, to remove all debris
31.
6. All accessibleradicular pulp is removed with the broach.
7. Canals are enlarged with the aim of removing all the
infected dentin and providing space for adequate
obturation.
8. Canals are irrigated with saline and dried. Paper points
are used for drying the canal walls.
9. Canals are then obturated with suitable resorbable
filling material
32.
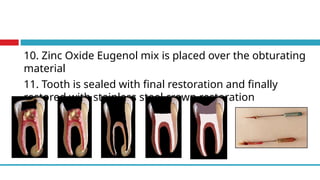
10. Zinc OxideEugenol mix is placed over the obturating
material
11. Tooth is sealed with final restoration and finally
restored with stainless steel crown restoration
33.
Multivisit Pulpectomy
▪ Usedfor non vital primary teeth with or without
associated abscess
▪ Clinical technique is similar to single visit
pulpectomy but all the procedures are not done
on the first visit.
▪ On the first visit pulp is extirpated, canals are
irrigated, dried and the tooth is temporarily
restored.
34.
▪ On thesecond visit the canals are enlarged and
if all the symptoms have subsided the tooth is
obturated and permanently restored.
▪ Obturation is postponed untill the symptoms
regresses.
▪ Between appointments, an antibacterial drug is
sealed in the pulp chamber
35.
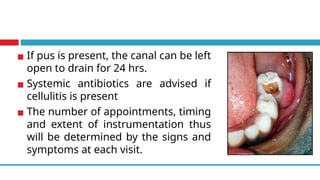
▪ If pusis present, the canal can be left
open to drain for 24 hrs.
▪ Systemic antibiotics are advised if
cellulitis is present
▪ The number of appointments, timing
and extent of instrumentation thus
will be determined by the signs and
symptoms at each visit.
36.
Radicular phase
1- Theremaining pulp tissue occupying the root canals is removed.
2- Canals are enlarged using endodontic file at a predetermined
working length, approximately 1 to 2 mm short of the root apices.
3- The canals should be enlarged several sizes beyond the size of
the first file that fits snugly into the canal to a minimum final size of
20 to 25.
4- Throughout root canal instrumentation, the canals should be
irrigated with sodium hypochlorite to aid in debridement.
37.
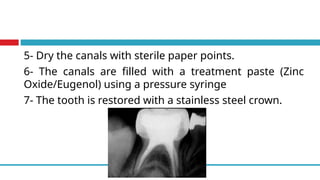
5- Dry thecanals with sterile paper points.
6- The canals are filled with a treatment paste (Zinc
Oxide/Eugenol) using a pressure syringe
7- The tooth is restored with a stainless steel crown.
Apexogenesis and Apexification
Openapex
⮚ At the time of tooth eruption root development is only
62-80% i.e., 2/3rd
of the root is formed.
⮚ If due to trauma or caries exposure the pulp
undergoes necrosis, dentin formation ceases and root
growth is arrested.
⮚ The resultant immature root will have an open apex
which is also called as blunder buss canal.
40.
Problems faced withopen apex
⮚ Due to large apical diameter and smaller coronal canal
diameter debridement is difficult.
⮚ Lack of apical stop makes obturation difficult.
⮚ The thin root canal walls become prone to fracture.
⮚ Earlier open apices have been treated by periapical surgery
with a retrograde filling but surgery has its drawbacks.
⮚ Relative to the already shortened root, further root reduction
(apicectomy) could result in an inadequate crown root ratio.
41.
⮚ The apicalwalls are thin and could shatter when
touched with a rotating bur.
⮚ The periapical tissue may not adapt to the wide and
irregular surface of the amalgam.
⮚ Surgery would remove the root sheath and prevent
for further root development.
⮚ Surgery would be both physically and psychologically
traumatic to the patient.
42.
❑ Thus Itis best to treat immature teeth with a non
surgical approach
❑ Based on the vitality of the pulp:
⮚ If the immature tooth has vital pulp exhibiting reversible
pulpitis physiological root end development or
apexogenesis is attempted.
⮚ If irreversible pulpitis is present there is when pulp is
necrotic then root apexification end closure is done by
Apexogenesis
◻Apexogenesis involves removalof the inflamed
pulp and the placement of calcium hydroxide
or MTA on the remaining healthy pulp tissue.
◻Traditionally this has implied removal of the
coronal portion of the pulp to permit continued
dentin formation and apical closure in an
immature tooth
Clinical Evaluation
✔No clinicalsymptoms
✔No radiogarphic changes in pulp or periapex
✔Continued root development
✔Radiographically observed hard tissue barrier
at the site of procedure
47.
Goals of apexogenesis
1.Continued development of root length for a more
favorable crown-to-root ratio.
2. Maintaining pulpal vitality
3. Promoting root end closure, thus creating a natural
apical constriction for root canal filling
Failures of apexogenesis
❖ Cessation of root growth
❖ Development of signs and symptoms or periapical
lesions
48.
Operative procedure
◻ Underlocal anaesthesia and rubber dam, pulp tissue is excised with a
diamond bur running at high speed under constant water cooling.
This causes least injury to the underlying pulp and is preferred to
hand excavation or the use of slow-speed steel burs.
◻ Microbial invasion of an exposed, vital pulp is usually superficial and
generally only 2-3 mm of pulp tissue should be removed (partial
pulpotomy)
◻ Removal of tissue may occasionally extend more deeply into the tooth
(full coronal pulpotomy) in an effort to preserve the apical portion of
the pulp and safeguard apical closure
49.
◻ Gently rinsethe wound with sterile saline or sodium hypochlorite (1-
2%) and remove any shredded tissue. All remaining tags of tissue in
the coronal portion must be removed as they may act as a nidus for
re-infection, and a pathway for coronal leakage
◻ Apply a calcium hydroxide dressing to the pulp to destroy any
remaining microorganism and to promote calcific repair.
◻ Overlay the calcium hydroxide dressing with a hard cement to
prevent its forceful injection into the pulp by chewing forces and a
final adhesive restoration which will seal the preparation against the
re-entry of microorganisms
50.
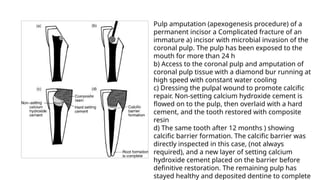
Pulp amputation (apexogenesisprocedure) of a
permanent incisor a Complicated fracture of an
immature a) incisor with microbial invasion of the
coronal pulp. The pulp has been exposed to the
mouth for more than 24 h
b) Access to the coronal pulp and amputation of
coronal pulp tissue with a diamond bur running at
high speed with constant water cooling
c) Dressing the pulpal wound to promote calcific
repair. Non-setting calcium hydroxide cement is
flowed on to the pulp, then overlaid with a hard
cement, and the tooth restored with composite
resin
d) The same tooth after 12 months ) showing
calcific barrier formation. The calcific barrier was
directly inspected in this case, (not always
required), and a new layer of setting calcium
hydroxide cement placed on the barrier before
definitive restoration. The remaining pulp has
stayed healthy and deposited dentine to complete
Apexification
is a methodof inducing apical closure through the
apexification formation mineralized tissue in apical pulp
region of a non vital tooth with an incompletely formed
root. The mineralized tissue can be osteodentin,
osteocementum, or bone or combination of all.
Indications
Restorable immature tooth with pulp necrosis
53.
Contraindications
1. All verticaland unfavourable horizontal root
fractures,
2. Resorptions
3. Periodontally broken down tooth
4. Vital pulp
54.
Objective:
The aim ofapexification is to induce either
closure of the open apical third of the root canal
or the formation of an apical “calcific barrier”
against which obturation can be achieved
55.
Rationale:
◻ The techniqueof treatment is the usual cleaning and
irrigation of the root canal, followed by sealing with a
paste of calcium hydroxide.
◻ Radiographic examination is made 3 and 6 months after
the procedure, and when evidence of a root apex cap or
barrier appears, the root canals are obturated. Actual root
growth does not occur as a result of apexification, but
radiographic evidence of a calcified mass at the root apex
gives that impression
56.
Materials used are:
1. Calcium hydroxide
2. Tricaclium phosphate
3. Bone growth factors
4. MTA
57.
Operative procedure
• Accesswith a high-speed, medium tapered fissure bur.
• Remove loose debris from the pulp chamber with hand
instruments, accompanied by copious, gentle irrigation with
sodium hypochlorite solution (1-2%)
• Canal preparation involve two processes: cleaning with
irrigants to free the root canal system of organic debris,
micro-organisms and their toxins; and shaping with enlarging
instruments, to modify the form of the existing canal to allow
the placement of a well-condensed root filling.
58.
• In canalswhich are often as wide as this, little dentine
removal and shaping is needed.
• Sodium hypochlorite solution (1-2%) as an irrigant will
continue dissolving organic debris and killing micro
organisms deep in the canal
• Working apically, files are directed around the canal walls
with a light rasping action to remove adherent debris.
Instrumentation is frequently punctuated by high volume,
low-pressure irrigation to flush .
59.
▪ Provisional workinglength should be 1 mm short of the
radiographic root apex. Further gentle filing and irrigation is then
continued to the definitive working length
▪ Dry canal with pre-measured paper points to avoid inadvertent over-
extension and damage to the periapical tissues
▪ Fill canal with a relatively calcium hydroxide paste such as. This may
be syringed into the canal via a disposable flexible tip. The
antimicrobial and mild tissue solvent activity of non-setting calcium
hydroxide will continue to cleanse the canal, and its high pH is
believed to encourage calcific root end closure
60.
• A radiographmay be taken to ensure a dense fill to
each root terminus
• Seal access cavity tightly between appointments to
prevent the leaching of calcium hydroxide, and
critically, to prevent the re-entry of micro-organisms
from the mouth which would disturb the process of
root end closure.
61.
Follow-up
◻Evaluation of signsand symptoms are made
regularly. Radiographs is taken once in 2-3
months, to evaluate the progress of barrier
formation
◻If the canal is closed, obturation may proceed. If
calcific barrier formation is not complete, the canal
should be redressed for a further 3 months.
Calcific barrier formation is usually complete
within 9-18 months, but could take up to 2 years
62.
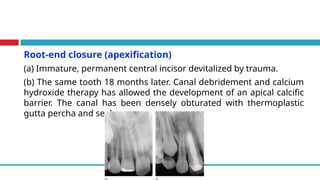
Root-end closure (apexification)
(a)Immature, permanent central incisor devitalized by trauma.
(b) The same tooth 18 months later. Canal debridement and calcium
hydroxide therapy has allowed the development of an apical calcific
barrier. The canal has been densely obturated with thermoplastic
gutta percha and sealer
63.
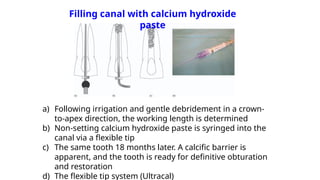
Filling canal withcalcium hydroxide
paste
a) Following irrigation and gentle debridement in a crown-
to-apex direction, the working length is determined
b) Non-setting calcium hydroxide paste is syringed into the
canal via a flexible tip
c) The same tooth 18 months later. A calcific barrier is
apparent, and the tooth is ready for definitive obturation
and restoration
d) The flexible tip system (Ultracal)
64.
Alternatives to theroot-end closure procedure
• Recently the potential has arisen to seal open apices with mineral
trioxide aggregate (MTA). Based on Portland building cement it is
packed into the canal with premeasured pluggers and sets to form a
hard, sealing, biocompatible barrier within 4 h
• Moist cotton wool is placed into the canal to promote setting and
the material is checked after at least 24 h before filling the
remainder of the canal with gutta percha and sealer
• Clinical studies are ongoing, but this material seems likely to allow
root end closure in 1 or 2 visits which will demand less patient
compliance
65.
• When pulpvitality is lost in an almost fully formed tooth,
it may be possible to avoid lengthy root-end closure
procedures by creating an apical stop against which a
root filling may be packed. Following crown to apex
preparation as described above, endodontic hand files
may be
• Alternatively, MTA can be packed into the apical 1-2 mm
of the canal with pluggers to provide an immediate apical
seal
66.
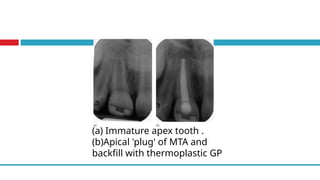
(a) Immature apextooth .
(b)Apical 'plug' of MTA and
backfill with thermoplastic GP