


























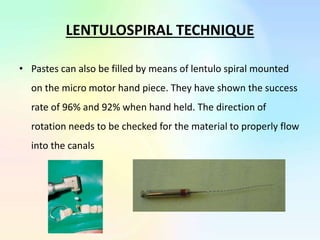







































This document provides information about pulpectomy procedures for primary teeth. It begins with definitions of pulpectomy and considerations for primary teeth. Indications include traumatized or carious primary teeth with signs of pain or infection, while contraindications include non-restorable teeth or excessive root resorption. The procedure involves accessing the pulp chamber, removing coronal and radicular pulp tissue, cleaning and shaping canals, and obturating with resorbable materials like zinc oxide eugenol. Access cavities must be carefully prepared and obturation techniques like lentulo spirals or pressure syringes are discussed. Success criteria include resolution of symptoms and adequate root length for exfoliation. Periodic reviews are



































































