Download to read offline
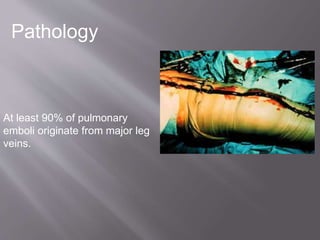
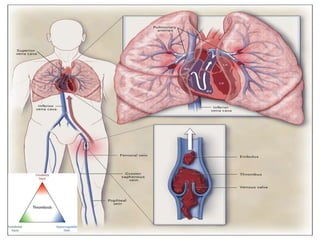
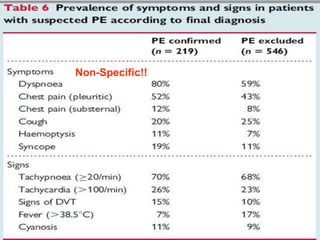

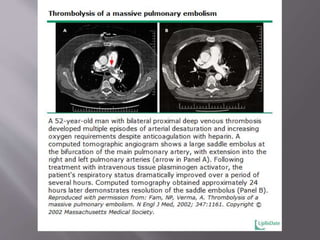
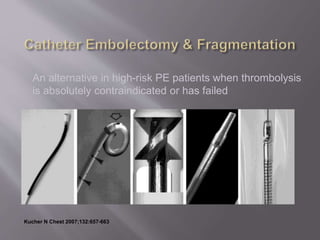
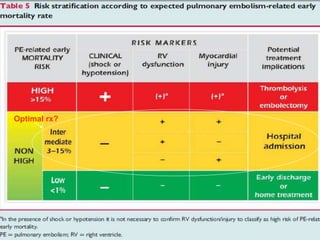
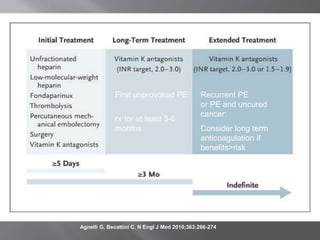


This document discusses pulmonary embolism (PE), including its causes, symptoms, diagnosis, and treatment. Some key points: - PE is a common cause of preventable death, often occurring without warning signs. Prompt diagnosis and treatment are important. - PE usually originates from blood clots that form in the deep leg veins. Symptoms can include chest pain, difficulty breathing, and syncope. - Diagnosis is difficult as symptoms are non-specific. Imaging tests like CT scans are often needed along with blood tests like d-dimers. - Treatment involves blood thinners to prevent further clots. Thrombolysis may be used in high-risk cases but risks need to be weighed








































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



