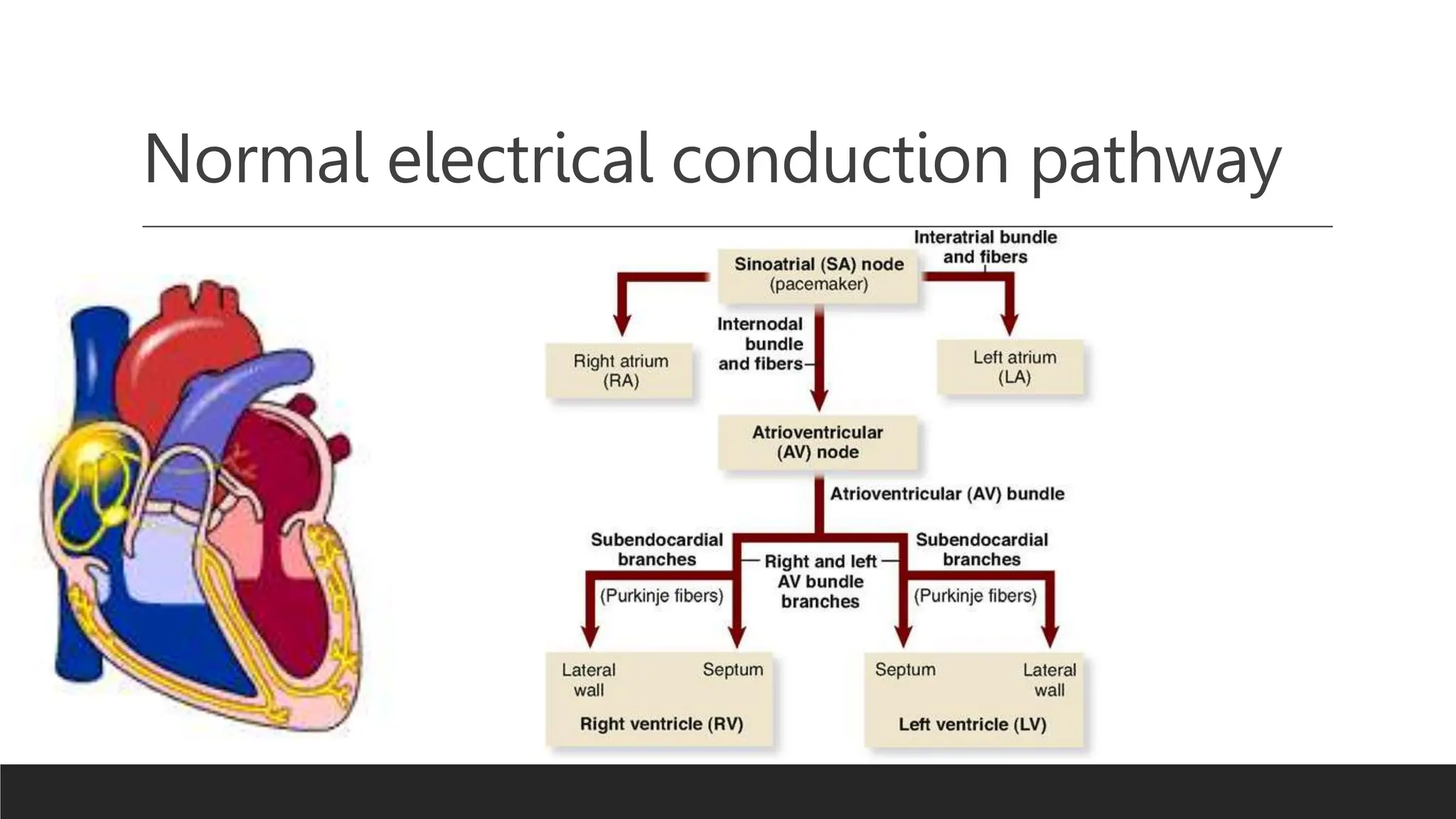
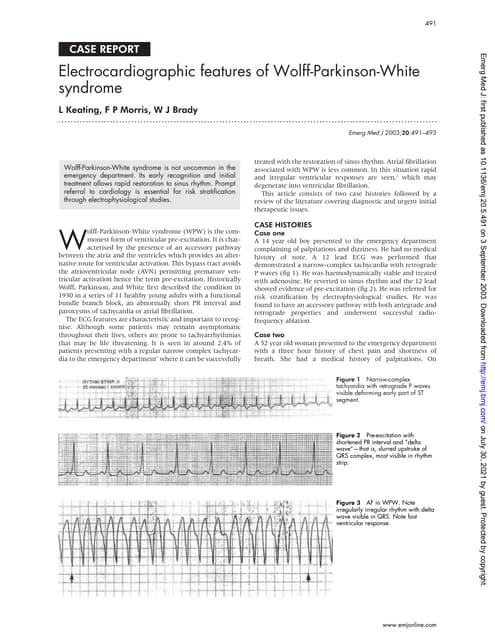
Ventricular preexcitation syndrome refers to abnormal accessory pathways in the heart's electrical system that bypass the normal conduction pathway. This leads to early activation of the ventricles seen on ECG as a short PR interval and delta wave. The most common forms are Wolff-Parkinson-White, Lown-Ganong-Levine, and Mahaim syndromes. While often congenital, it can also be associated with genetic mutations, structural heart defects, age and gender. Management involves monitoring, medications, catheter ablation to destroy accessory pathways, and educating patients on symptoms and emergency preparedness.