Primary open angle glaucoma
•Download as PPTX, PDF•
9 likes•272 views

POAG, its clinical signs, investigations and treatment.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Primary open angle glaucoma
Similar to Primary open angle glaucoma (20)
More from faculty of medicine -benha university
More from faculty of medicine -benha university (20)
Recently uploaded
Recently uploaded (20)
Primary open angle glaucoma
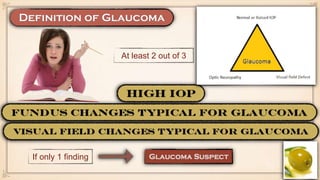
- 1. At least 2 out of 3 If only 1 finding
- 3. • Disturbance of the structural or functional integrity of the optic nerve, in which; IOP > 21 mmHg Glaucomatous ONH damage Characteristic visual field changes Open AC angle Absent signs of 2ry glaucoma or a non glaucomatous cause of optic neuropathy
- 4. • The higher the IOP, the greater the likelihood of glaucoma • More common in old age • More common in Black individuals • Siblings, offspring • More common in Myopic individuals • Hypertension, Diabetes, Migraine
- 5. • Direct mechanical damage to RNF • Ischaemic damage
- 6. • Nothing • Except in late cases when the patient complains of restricted visual field • Steroids (elevates IOP), ℬ blockers e.g. for hypertension (lowers IOP) • Trauma, surgery, inflammation • Cardiovascular, respiratory disease; for proper tailoring of medications
- 7. • Phasing (Note time of the day), Asymmetry • C/D ratio (Asymmetry), Peri papillary area, RNFL defect • Not affected except in advanced cases • Not affected except in advanced cases (RAPD in post glaucomatous OA) • Open angle • To exclude causes of 2ry glaucoma
- 8. • Measure IOP while the patient is fasting • Drink 1 litre over 5 - 15 minutes • Measure IOP subsequently every 15 minutes for one hour • A rise in IOP of 6 to 8 mmHg or an increase from baseline of 30% or more at any time during the hour was considered a positive test.
- 9. • To adjust the IOP reading according to the central corneal thickness. • Pseudo-colour map of ONH & peri-papillary RNFL thickness. • The visual field defect corresponds to the pattern of fibres in the retinal area served
- 10. مهمجدا • can form at a relatively early stage, often superonasally from the earliest to the latest
- 11. •the defect is bounded by the horizontal midline, corresponding to the retinal nerve fibre layer horizontal raphe.
- 12. •Less common than nasal step, WHY?!!
- 13. •Develop from coalescent para-central scotomas •Baring of the blind spot = extension from the blind spot around fixation
- 15. • Develops when superior and inferior arcuate defects become continuous
- 16. • A small island of central vision
- 17. • 1ry vs 2ry glaucoma • Causes of visual field defects mimic glaucoma field defects e.g. ONH drusen, tilted ONH • Prevent functional impairment of vision within the patient’s lifetime by slowing the rate of ganglion cell loss closer to that of the normal population.
- 18. • Increases uveoscleral outflow • Increases trabecular outflow • Latanoprost • Once daily at bed time • Conjunctival hyperaemia • Eye lash thickening, lengthening & hyper pigmentation • Irreversible iris hyper pigmentation • Peri ocular skin hyper pigmentation • Cystoid macular edema • Promotion of herpetic keratitis • Anterior uveitis • Travaprost • Bimatoprost
- 19. • Decreases aqueous production by ciliary epithelium • Timolol • Twice daily (not at bed time to avoid profound hypotension) • Ocular: Allergy, PEE • Systemic: 1. Bronchospasm; contraindicated in asthmatic patients 2. Bradycardia, Hypotension, Heart block, Heart failure 3. Dyslipidemia, headache, decrease lipido • Betaxolol (increases ON blood flow) • Levobunolol
- 20. • Decreases aqueous production by ciliary epithelium • Increases uveoscleral outflow • Brimonidine • Twice daily • Ocular: Allergic conjunctivitis • Systemic: 1. Xerostomia 2. Cross the blood brain barrier (CI under the age of 2 years) • Apraclonidine
- 21. • Decreases aqueous production by ciliary epithelium • Dorzolamide • Twice daily • Ocular: Allergic blepharo-conjunctivitis • Systemic: 1. Idiosyncrasy (Bone marrow suppression) • Brinzolamide
- 22. •improve convenience and patient compliance •more cost effective • Timolol + Dorzolamide (Cosopt) • Timolol + Travaprost (Duotrav) • Timolol + Brimonidine (Combigan)
- 23. • Decreases aqueous production by ciliary epithelium • Acetazolmide • Used for control of acute attack of glaucoma with high IOP • Ocular: Choroidal effusion • Systemic: 1. Paraesthesia 2. Renal stones 3. GIT disturbances 4. Malaise
- 24. •Create an osmotic gradient so that water is ‘drawn out’ from the vitreous into the blood • Mannitol (IV) • Used for control of acute attack of glaucoma with high IOP • Systemic: 1. Cardiovascular overload 2. Urine retention 3. Headache • Glycerol (Oral) • Isosorbide (Oral)
- 25. • Beta blockers • CAI • Alpha 2 agonists • PG derivatives • Alpha 2 agonists
- 26. • Start with single line (usually PG derivative or Beta blocker) • Choose the drug with fewest side effects, lowest concentration • Usually after 2-4 weeks • Response to the drug is assessed against the desired target IOP • Target IOP is tailored according to the patient: Age Presenting IOP ONH changes Field defects
- 27. • Subsequent assessment is set for further 3-6 months • ONH exam is done in each visit • Perimetry is done every 6-12 months • Gonioscopy is done every 12 months as AC angle tend to narrow with age • Patient compliance • Proper target IOP setting • Diurnal variation
- 28. • Substitute to another drug, then review • Add another drug or use fixed combination Laser trabeculoplasty (LTP) involves the delivery of laser to the trabecular meshwork with the aim of enhancing aqueous outflow and thereby lowering IOP.
- 29. ALT SLT LASER Argon Nd YAG Mechanism of action Thermal damage to TM, leading to mechanical opening of TM spaces Selectively target melanin pigment in trabecular meshwork (TM) cells, leaving non-pigmented structures unscathed. Repeatability Not repeatable Could be repeated Electron Microscopy of TM
- 30. • Poorly controlled POAG with medical or laser therapy • Poor compliance with medical treatment • Advanced POAG requiring very low target IOP • To create a fistula between the AC & the sub-conjunctival space from which the aqueous drains.
- 32. • Blebitis, Endophthalmitis • Treatment; IV Fortified antibiotics (Vancomycin + Ceftazidime), Vitrectomy
- 33. • With Deep AC >> Filed bleb (Sub-conjunctival fibrosis) • With Shallow AC >> Pupillary Block >> Malignant Glaucoma (Aqueous misdirection)
- 34. • With Deep AC >> Choroidal detachment • With Shallow AC >> Over Filtration >> Bleb Leak
- 36. •In non-penetrating filtration surgery the AC is not entered and the internal trabecular meshwork is preserved, thus reducing the incidence of postoperative over filtration with hypotony & its potential sequelae. •Two concentric lamellar scleral flaps are fashioned & the deep flap excised leaving behind a thin membrane consisting of trabeculum/Descemet membrane through which aqueous diffuses from the AC to the subconjunctival space.