Downloaded 20 times



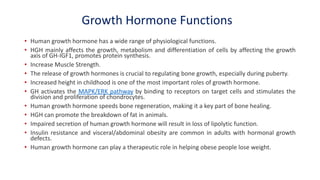









This document discusses the diagnosis of growth hormone deficiency (GHD). It begins by outlining the objectives which are an introduction to short stature, indications for GHD investigations, GH testing methods including physiological and pharmacological tests, and international criteria for GHD diagnosis. It then provides details on the GH gene and physiological GH secretion patterns controlled by GHRH and somatostatin. The functions of GH and IGF/IGFBP systems are described. Various GH stimulation tests including pharmacological tests using insulin, L-dopa, arginine and GHRH are outlined. International criteria for GHD diagnosis incorporate auxological parameters, biochemical markers, and subnormal responses to provocative tests.























































































