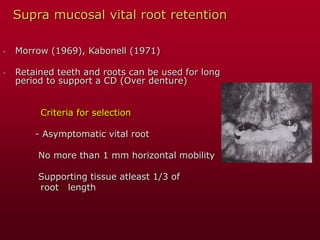
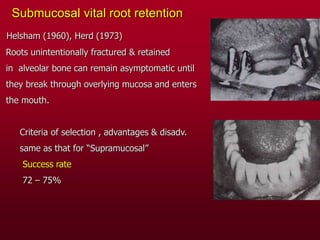
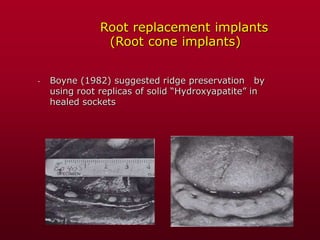
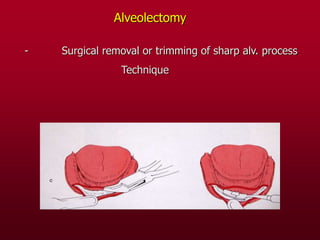
Preprosthetic surgery involves surgical procedures to enhance the denture-bearing area for better prosthetic support, masticatory function, and esthetics, while preserving tissue. It includes basic and advanced techniques, categorized by initial and secondary procedures, focusing on hard and soft tissue evaluations for ideal denture support. Key procedures involve ridge preservation, correction, and vestibuloplasty to improve the oral environment for prosthetic appliances.










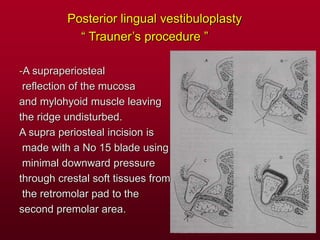
![Posterior lingual vestibuloplasty
“ Obwegesser’s procedure ”
[ Skin graft labiobuccal vest. + Trauner’s FOM plasty ]](https://image.slidesharecdn.com/prepros-240707094959-f4e7b646/85/preprosthetic-surgery-hard-and-soft-tissue-ppt-82-320.jpg)























![[1][m] minimally invasive restorative dentistry](https://cdn.slidesharecdn.com/ss_thumbnails/1mminimallyinvasiverestorativedentistry-160422162403-thumbnail.jpg?width=640&height=640&fit=bounds)




































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)






