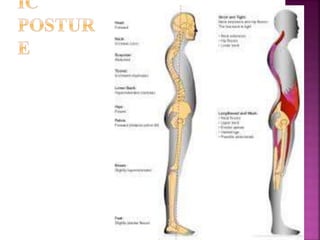
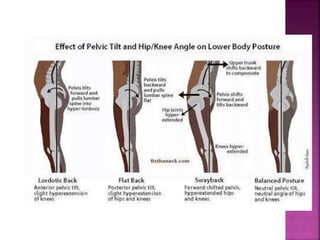
This document discusses various aspects of posture including definitions of different types of posture, muscle involvement in maintaining posture, postural reflexes, factors affecting posture, and descriptions and causes of some common postural deviations like kyphosis, lordosis, scoliosis, etc. Key points include:
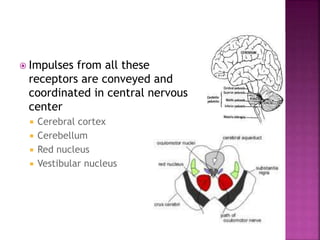
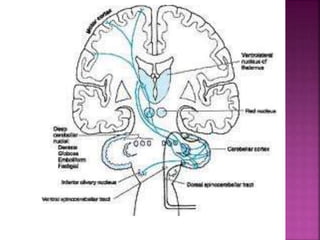
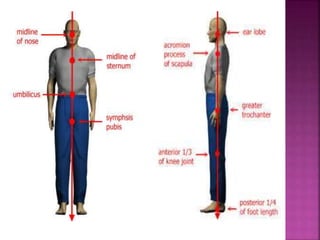
- Posture is the body position maintained by muscle activity and reflexes in response to stimuli from muscles, eyes, ears and joints. Both static and dynamic posture involve integration of postural reflexes.
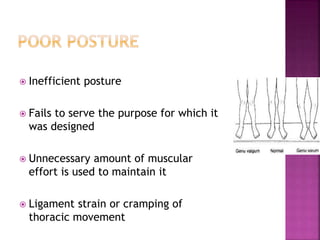
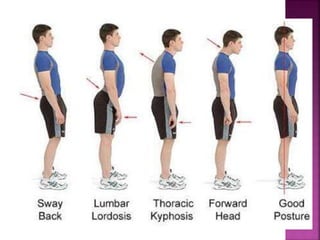
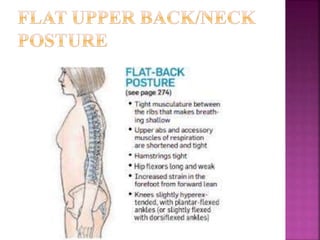
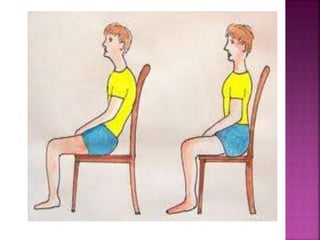
- Good posture allows maximum efficiency with minimal effort while poor posture causes unnecessary muscle strain and reduces function.
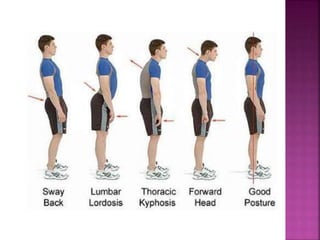
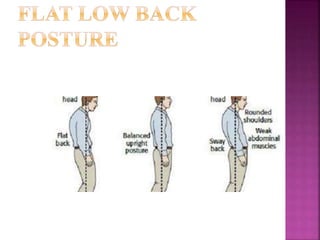
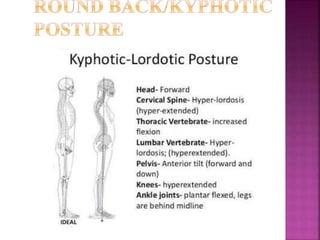
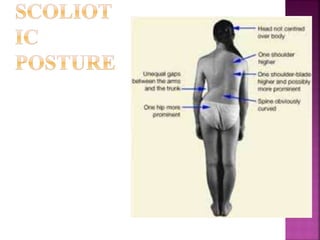
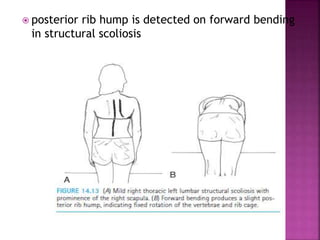
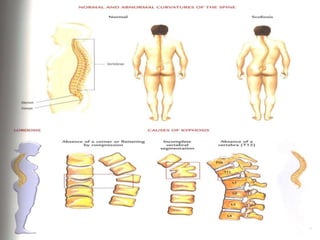
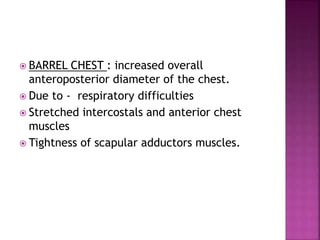
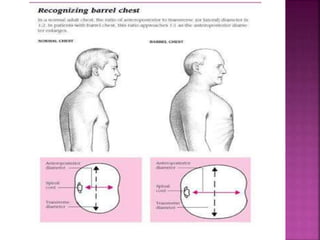
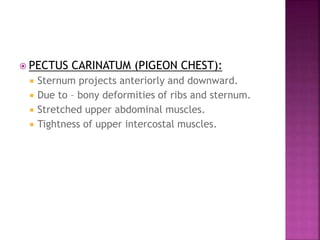
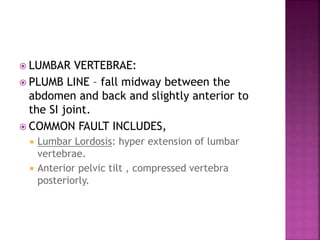
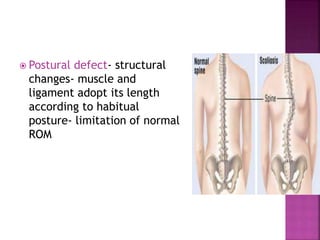
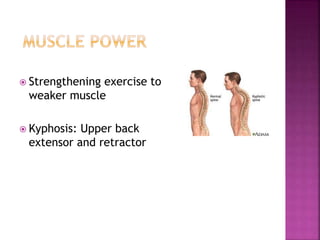
- Common postural deviations include kyphosis (rounded back), lordosis (swayback), and scoliosis




































![Posture- Physical Therapy [VNSGU]](https://cdn.slidesharecdn.com/ss_thumbnails/posture-180915145350-thumbnail.jpg?width=640&height=640&fit=bounds)








![Waves Ultimate 15 v24.11.17 With Crack for MacOS [Latest ]](https://cdn.slidesharecdn.com/ss_thumbnails/presentationonposture-250409203259-21999cb1-250409210017-8d703091-thumbnail.jpg?width=640&height=640&fit=bounds)


![Freemake Video Converter Crack + Serial Key [Latest]](https://cdn.slidesharecdn.com/ss_thumbnails/presentationonposture-250409203259-21999cb1-250409205402-3ea828f6-thumbnail.jpg?width=640&height=640&fit=bounds)

![CyberLink PhotoDirector Ultra Crack Free Download [Latest] 2025](https://cdn.slidesharecdn.com/ss_thumbnails/presentationonposture-250409203259-21999cb1-250409211238-0f15f8fb-thumbnail.jpg?width=640&height=640&fit=bounds)






































