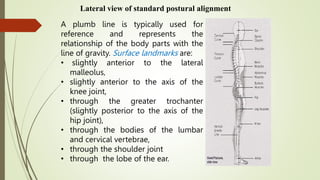
Posture refers to the alignment of the body parts and is influenced by many factors. The spine has four curves - two primary curves in the posterior direction and two compensatory curves in the anterior direction. Good postural alignment involves maintaining a plumb line that passes through the body's surface landmarks. Posture is maintained through the interaction of the passive structures like bones and ligaments, active muscles, and neural control. Factors like age, pregnancy, occupation, handedness, muscle tightness/weakness, and obesity can impact one's posture. Developing good postural habits is important to avoid pain and dysfunction.
















































![CyberLink PhotoDirector Ultra Crack Free Download [Latest] 2025](https://cdn.slidesharecdn.com/ss_thumbnails/presentationonposture-250409203259-21999cb1-250409211238-0f15f8fb-thumbnail.jpg?width=640&height=640&fit=bounds)

![Freemake Video Converter Crack + Serial Key [Latest]](https://cdn.slidesharecdn.com/ss_thumbnails/presentationonposture-250409203259-21999cb1-250409205402-3ea828f6-thumbnail.jpg?width=640&height=640&fit=bounds)

![Waves Ultimate 15 v24.11.17 With Crack for MacOS [Latest ]](https://cdn.slidesharecdn.com/ss_thumbnails/presentationonposture-250409203259-21999cb1-250409210017-8d703091-thumbnail.jpg?width=640&height=640&fit=bounds)















































