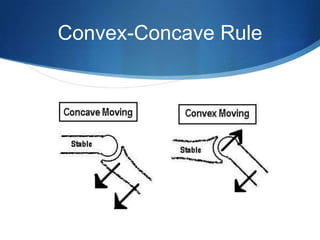
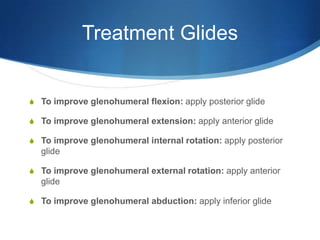
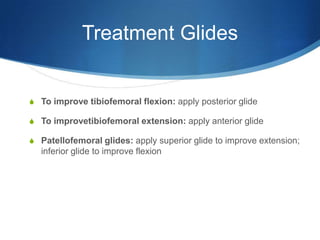
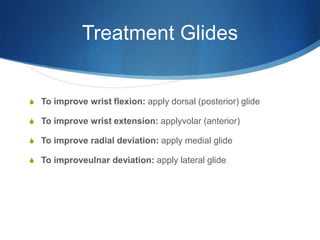
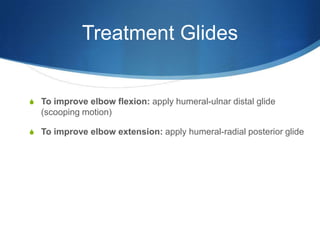
The document discusses principles of joint mobilization including using lower grades to reduce pain and higher grades to increase mobility. It outlines convex-concave rules for determining glide direction in different joints. Treatment glides are described to improve range of motion in various joints like the shoulder, knee, ankle and elbow. Open-packed positions and grades of movement are also defined. The goal of a joint mobilization treatment is to increase range of motion through appropriate gliding techniques.