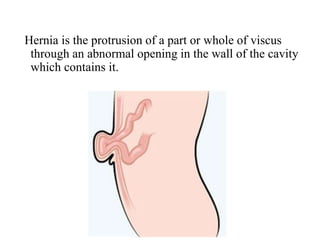
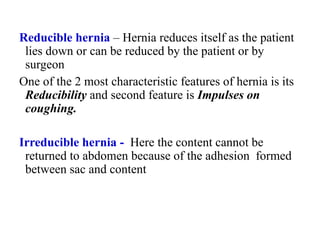
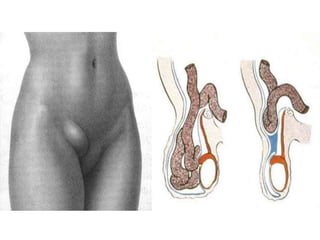
Hernias occur when an internal organ or tissue protrudes through a weakness in the muscle or surrounding wall of the cavity it normally resides in. The most common types of external hernias are inguinal, femoral, and umbilical hernias. Hernias can be classified as reducible, irreducible, obstructed, or strangulated depending on whether the protruding tissue can be pushed back into place and if blood flow is restricted. Treatment options include herniorrhaphy to surgically repair the weak area and physiotherapy to strengthen muscles and prevent recurrence.









































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



