

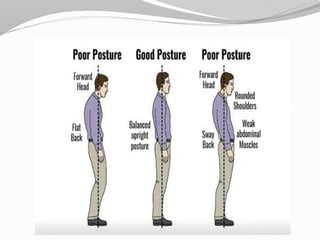




This document discusses posture and postural alignment. It defines posture and describes the development of spinal curvature from birth. Good posture is defined as a position with stability, balance and minimal effort. Poor posture results from deviations from good alignment. Factors like muscles, nerves, reflexes and the central nervous system contribute to postural control. Techniques for assessing and correcting posture include exercises, stretching, strengthening, taping and myofascial release. Maintaining mobility, muscle balance and retraining awareness can help improve poor posture.

































![Posture- Physical Therapy [VNSGU]](https://cdn.slidesharecdn.com/ss_thumbnails/posture-180915145350-thumbnail.jpg?width=640&height=640&fit=bounds)







































