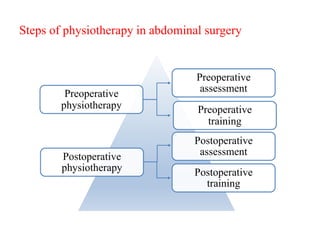
Physiotherapy plays an important role in the pre and post operative stages of abdominal surgery to prevent pulmonary and circulatory complications. Preoperative physiotherapy includes assessment, education, and training patients in breathing and coughing exercises. Postoperative physiotherapy focuses on further exercises and mobilization to aid recovery and reduce complications like pneumonia, pain management, and scar tissue prevention. Studies show preoperative training and post operative chest physiotherapy can reduce hospital stays and improve outcomes for surgery patients.

![• The various techniques of physiotherapy (chest physiotherapy,
incentive spirometry, continuous positive airway pressure
breathing) seem to be equivalent in efficacy; but intermittent
positive pressure breathing has no advantages, compared with
the other treatments and could even be deleterious. Chest
physiotherapy and incentive spirometry are the most practical
methods available for decreasing secretion contents of
airways, whereas continuous positive airway pressure
breathing is efficient on atelectasis.
• Rezaiguia S, Jayr C. [Prevention of respiratory complications after abdominal
surgery] Annales Francaises D'anesthesie et de Reanimation. 1996 ;15(5):623-646.](https://image.slidesharecdn.com/preandpostpt-kk3-221214102712-9f14f37f/85/pre-and-post-PT-kk-3-pptx-28-320.jpg)









![Neurophysiological facilitation of respiration [npf]](https://cdn.slidesharecdn.com/ss_thumbnails/neurophysiologicalfacilitationofrespirationnpf-180714163516-thumbnail.jpg?width=640&height=640&fit=bounds)





































































