Downloaded 688 times

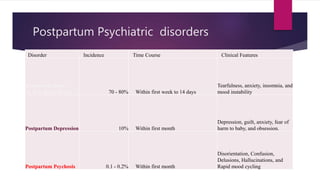

Postpartum depression (PPD) is a mood disorder that typically occurs within the first few weeks after childbirth and can last up to a year if untreated, affecting about 10% of new mothers. It is characterized by symptoms such as depression, anxiety, and intrusive thoughts, with risk factors including a history of depression, stressful events during pregnancy, and complications during birth. Treatment options include antidepressants, cognitive behavioral therapy, and support resources for both mothers and fathers, as PPD can also affect men, especially when correlated with partners' mental health.













































![Post Partum Disorders [2001]](https://cdn.slidesharecdn.com/ss_thumbnails/postpartum-170814005829-thumbnail.jpg?width=640&height=640&fit=bounds)

































