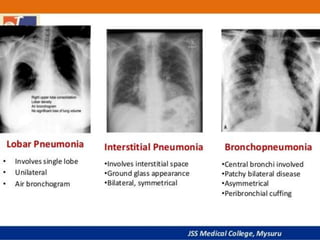
Pneumonia is a lung infection characterized by inflammation and fluid in the alveoli, which can make breathing difficult. It poses a significant health risk, particularly to older adults and those with weakened immune systems, with many hospitalizations and fatalities reported in developed nations. Treatment typically involves antibiotics, rest, and supportive care, while prevention strategies include vaccination and improved nutrition.















![
Oral antibiotics, rest , simple analgesics, fluids
Antibiotics- Amoxicillin ,doxycycline ,clarithromycin
The duration of treatment has traditionally been seven to
ten days
Neuraminidase inhibitors may be used to treat viral
pneumonia caused by influenza viruses (influenza A and
influenza B).
Influenza A may be treated with rimantadine or
amantadine, while influenza A or B may be treated with
oseltamivir, zanamivir or peramivir.[11] These are of most
benefit if they are started within 48 hours of the onset of
symptoms
MANAGEMENT/ TREATMENT](https://image.slidesharecdn.com/pneumonia-180507154759/85/Pneumonia-25-320.jpg)