PNEUMONIA
•Pneumonia is definedas acute inflammation of the
lung parenchyma distal to the terminal bronchioles
(consisting of the respiratory bronchiole, alveolar
ducts, alveolar sacs and alveoli).
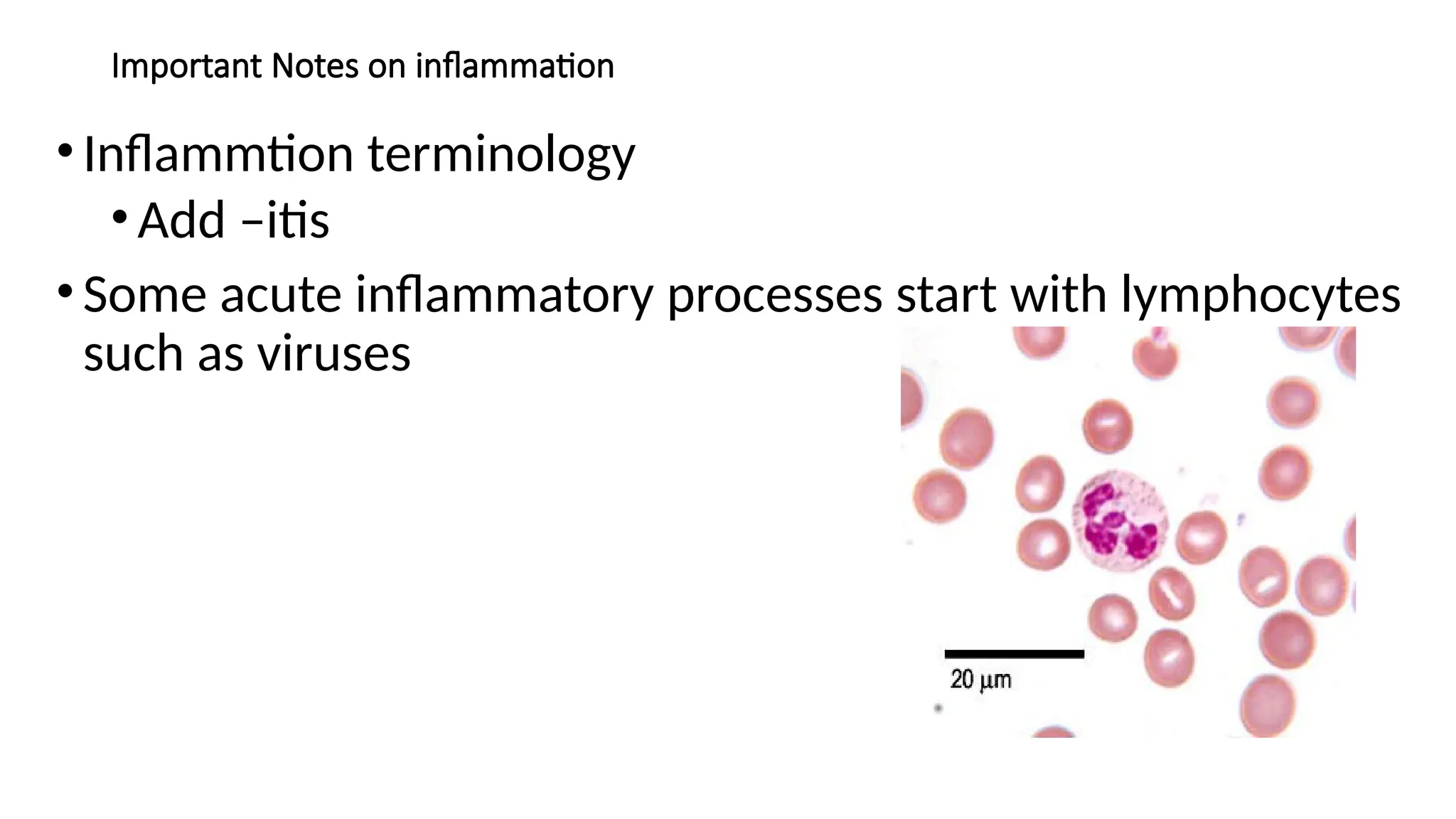
•The terms ‘pneumonia’ and ‘pneumonitis’ are often
used synonymously for inflammation of the lungs,
while ‘consolidation’ (meaning solidification) is the
term used for gross and radiologic appearance of the
lungs in pneumonia
6.
ENTRY
•The microorganisms gainentry into the lungs by one
of the following four routes:
i. Inhalation of the microbes present in the air.
ii. Aspiration of organisms from the nasopharynx or
oropharynx.
iii. Haematogenous spread from a distant focus of
infection.
iv. Direct spread from an adjoining site of infection.
7.
PATHOGENESIS
•The normal lungis free of bacteria because of the
presence of a number of lung defense mechanisms at
different levels such as nasopharyngeal filtering
action, mucociliary action of the lower respiratory
airways, the presence of phagocytosing alveolar
macrophages and immunoglobulins.
•Failure of these defense mechanisms and presence of
certain predisposing factors result in pneumonias.
•These conditions are as under;
8.
•1. Altered consciousness.The oropharyngeal contents may
be aspirated in states causing unconsciousness e.g. in coma,
cranial trauma, seizures, cerebrovascular accidents, drug
overdose, alcoholism etc.
•2. Depressed cough and glottic reflexes. Depression of
effective cough may allow aspiration of gastric contents e.g.
in old age, pain from trauma or thoracoabdominal surgery,
neuromuscular disease, weakness due to malnutrition,
kyphoscoliosis, severe obstructive pulmonary diseases,
endotracheal intubation and tracheostomy.
9.
•3. Impaired mucociliarytransport. The normal protection
offered by mucus-covered ciliated epithelium in the airways
from the larynx to the terminal bronchioles is impaired or
destroyed in many conditions favouring passage of bacteria
into the lung parenchyma. These conditions are cigarette
smoking, viral respiratory infections, immotile cilia
syndrome, inhalation of hot or corrosive gases and old age.
•4. Impaired alveolar macrophage function. Pneumonias
may occur when alveolar macrophage function is impaired
e.g. by cigarette smoke, hypoxia, starvation, anaemia,
pulmonary oedema and viral respiratory infections.
10.
•5. Endobronchial obstruction.The effective
clearance mechanism is interfered in
endobronchial obstruction from tumour, foreign
body, cystic fibrosis and chronic bronchitis.
•6. Leucocyte dysfunctions. Disorders of
lymphocytes including congenital and acquired
immunodeficiencies (e.g. AIDS,
immunosuppressive therapy) and granulocyte
abnormalities may predispose to pneumonia.
11.
CLASSIFICATION
• On thebasis of the anatomic part of the lung parenchyma involved,
pneumonias are traditionally classified into 3 main types:
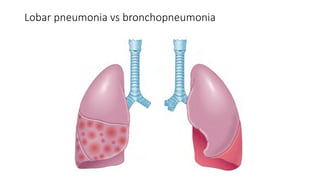
1. Lobar pneumonia
2. Bronchopneumonia (or Lobular pneumonia)
3. Interstitial pneumonia.
• Or depending on the etiology;pneumonias into following 3 main groups:
A. Bacterial pneumonia
B. Viral pneumonia
C. Pneumonias from other etiologies.
• In this lecture, a combined approach of etiologic and morphologic
classification will be followed
BACTERIAL PNEUMONIA
• Bacterialinfection of the lung parenchyma is the most common
cause of pneumonia or consolidation of one or both the lungs.
• Two types of acute bacterial pneumonias are distinguished—
lobar pneumonia and broncho-(lobular-) pneumonia, each with
distinct etiologic agent and morphologic changes.
• Another type distinguished by some workers separately is
confluent pneumonia which combines the features of both lobar
and bronchopneumonia and involves larger (confluent) areas in
both the lungs irregularly, while others consider this as a variant
of bronchopneumonia.
14.
LOBAR PNEUMONIA
•Lobar pneumoniais an acute bacterial
infection of a part of a lobe, the entire
lobe, or even two lobes of one or both
the lungs.
15.
ETIOLOGY.
• Based onthe etiologic microbial agent causing lobar pneumonia,
following types of lobar pneumonia are described:
• 1. Pneumococcal pneumonia. More than 90% of all lobar
pneumonias are caused by Streptococcus pneumoniae,
• Pneumococcal pneumonia in majority of cases is community-
acquired infection
• 2. Staphylococcal pneumonia. Staphylococcus aureus causes
pneumonia by haematogenous spread of infection from another
focus or after viral infections.
16.
•3. Streptococcal pneumonia.β-haemolytic streptococci
may rarely cause pneumonia such as in children after
measles or influenza, in severely debilitated elderly
patients and in diabetics.
•4. Pneumonia by gram-negative aerobic bacteria. Less
common causes of lobar pneumonia are gram-negative
bacteria like Haemophilus influenzae, Klebsiella
pneumonia, Pseudomonas, Proteus and Escherichia coli.
• H. influenzae commonly causes pneumonia in children
below 3 years of age after a preceding viral infection.
17.
MORPHOLOGIC FEATURES.
• Laennec’soriginal description divides lobar pneumonia into 4
sequential pathologic phases: stage of congestion (initial phase),
red hepatisation (early consolidation), grey hepatisation (late
consolidation) and resolution.
• However, these classic stages seen in untreated cases are found
much less often nowadays due to early institution of antibiotic
therapy and improved medical care.
• In lobar pneumonia, as the name suggests, part of a lobe, a whole
lobe, or two lobes are involved, sometimes bilaterally. The lower
lobes are affected most commonly.
18.
• The sequenceof pathologic changes described below represents the
inflammatory response of lungs in bacterial infection;
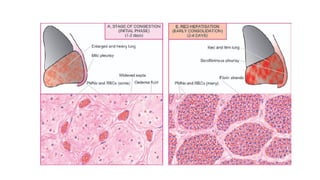
• 1. STAGE OF CONGESTION: INITIAL PHASE
• The initial phase represents the early acute inflammatory response to
bacterial infection and lasts for 1 to 2 days.
• Grossly, the affected lobe is enlarged, heavy, dark red and congested. Cut
surface exudes blood-stained frothy fluid.
• Histologically, typical features of acute inflammatory response to the
organisms are seen. These are as under
• i) Dilatation and congestion of the capillaries in the alveolar walls.
• ii) Pale eosinophilic oedema fluid in the air spaces.
• iii) A few red cells and neutrophils in the intra-alveolar fluid.
• iv) Numerous bacteria demonstrated in the alveolar fluid by Gram’s staining.
19.
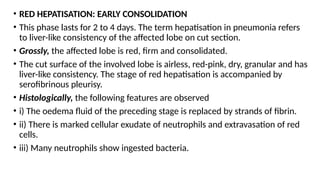
• RED HEPATISATION:EARLY CONSOLIDATION
• This phase lasts for 2 to 4 days. The term hepatisation in pneumonia refers
to liver-like consistency of the affected lobe on cut section.
• Grossly, the affected lobe is red, firm and consolidated.
• The cut surface of the involved lobe is airless, red-pink, dry, granular and has
liver-like consistency. The stage of red hepatisation is accompanied by
serofibrinous pleurisy.
• Histologically, the following features are observed
• i) The oedema fluid of the preceding stage is replaced by strands of fibrin.
• ii) There is marked cellular exudate of neutrophils and extravasation of red
cells.
• iii) Many neutrophils show ingested bacteria.
20.
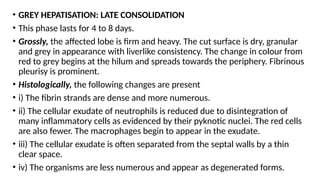
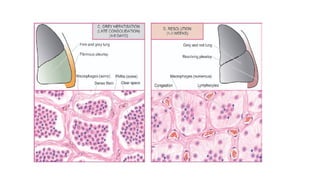
• GREY HEPATISATION:LATE CONSOLIDATION
• This phase lasts for 4 to 8 days.
• Grossly, the affected lobe is firm and heavy. The cut surface is dry, granular
and grey in appearance with liverlike consistency. The change in colour from
red to grey begins at the hilum and spreads towards the periphery. Fibrinous
pleurisy is prominent.
• Histologically, the following changes are present
• i) The fibrin strands are dense and more numerous.
• ii) The cellular exudate of neutrophils is reduced due to disintegration of
many inflammatory cells as evidenced by their pyknotic nuclei. The red cells
are also fewer. The macrophages begin to appear in the exudate.
• iii) The cellular exudate is often separated from the septal walls by a thin
clear space.
• iv) The organisms are less numerous and appear as degenerated forms.
21.
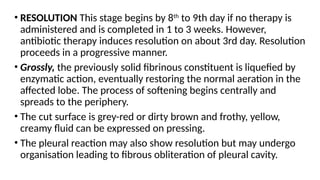
• RESOLUTION Thisstage begins by 8th
to 9th day if no therapy is
administered and is completed in 1 to 3 weeks. However,
antibiotic therapy induces resolution on about 3rd day. Resolution
proceeds in a progressive manner.
• Grossly, the previously solid fibrinous constituent is liquefied by
enzymatic action, eventually restoring the normal aeration in the
affected lobe. The process of softening begins centrally and
spreads to the periphery.
• The cut surface is grey-red or dirty brown and frothy, yellow,
creamy fluid can be expressed on pressing.
• The pleural reaction may also show resolution but may undergo
organisation leading to fibrous obliteration of pleural cavity.
22.
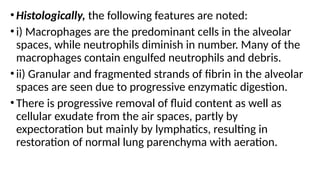
•Histologically, the followingfeatures are noted:
•i) Macrophages are the predominant cells in the alveolar
spaces, while neutrophils diminish in number. Many of the
macrophages contain engulfed neutrophils and debris.
•ii) Granular and fragmented strands of fibrin in the alveolar
spaces are seen due to progressive enzymatic digestion.
•There is progressive removal of fluid content as well as
cellular exudate from the air spaces, partly by
expectoration but mainly by lymphatics, resulting in
restoration of normal lung parenchyma with aeration.
25.
COMPLICATIONS.
•Since the adventof antibiotics, serious complications of
lobar pneumonia are uncommon. However, they may
develop in neglected cases and in patients with impaired
immunologic defenses. These are as under:
•1. Organisation. In about 3% of cases, resolution of the
exudate does not occur but instead it undergoes
organisation.
•There is ingrowth of fibroblasts from the alveolar septa
resulting in fibrosed, tough, airless leathery lung tissue. This
type of post-pneumonic fibrosis is called carnification.
26.
•2. Pleural effusion.About 5% of treated cases of
lobar pneumonia develop inflammation of the pleura
with effusion.
•The pleural effusion usually resolves but sometimes
may undergo organisation with fibrous adhesions
between visceral and parietal pleura.
•3. Empyema. Less than 1% of treated cases of lobar
pneumonia develop encysted pus in the pleural
cavity termed empyema.
27.
•4. Lung abscess.A rare complication of lobar
pneumonia is formation of lung abscess, especially
when there is secondary infection by other organisms.
•5. Metastatic infection. Occasionally, infection in the
lungs and pleural cavity in lobar pneumonia may extend
into the pericardium and the heart causing purulent
pericarditis, bacterial endocarditis and myocarditis.
•Other forms of metastatic infection encountered rarely
in lobar pneumonias are otitis media, mastoiditis,
meningitis, brain abscess and purulent arthritis.
28.
CLINICAL FEATURES.
•Classically, theonset of lobar pneumonia is sudden.
The major symptoms are: shaking chills, fever,
malaise with pleuritic chest pain, dyspnoea and
cough with expectoration which may be mucoid,
purulent or even bloody.
•The common physical findings are fever, tachycardia,
and tachypnoea, and sometimes cyanosis if the
patient is severely hypoxaemic.
•There is generally a marked neutrophilic leucocytosis.
Blood cultures are positive in about 30% of cases.
29.
DIAGNOSIS AND TREATMENT
•Chestradiograph may reveal consolidation.
•Culture of the organisms in the sputum and
antibiotic sensitivity are most significant
investigations for institution of specific antibiotics.
•The response to antibiotics is usually rapid with
clinical improvement in 48 to 72 hours after the
initiation of antibiotics
30.
BRONCHOPNEUMONIA
•Bronchopneumonia is infectionof the terminal
bronchioles that extends into the surrounding alveoli
resulting in patchy consolidation of the lung.
•The condition is particularly frequent at the
extremes of life (i.e. in infancy and old age), as a
terminal event in chronic debilitating diseases and as
a secondary infection following viral respiratory
infections such as influenza, measles etc.
31.
ETIOLOGY.
•The common organismsresponsible for
bronchopneumonia are staphylococci,
streptococci, pneumococci, Klebsiella
pneumoniae, Haemophilus influenzae, and gram-
negative bacilli like Pseudomonas and coliform
bacteria
32.
MORPHOLOGIC FEATURES
•Grossly, bronchopneumoniais identified by patchy areas of
red or grey consolidation affecting one or more lobes,
frequently found bilaterally and more often involving the
lower zones of the lungs due to gravitation of the
secretions.
•On cut surface, these patchy consolidated lesions are dry,
granular, firm, red or grey in colour, 3 to 4 cm in diameter,
slightly elevated over the surface and are often centred
around a bronchiole
•These patchy areas are best picked up by passing the
fingertips on the cut surface
33.
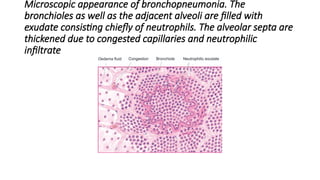
•Histologically, the followingfeatures are observed
•i) Suppurative exudate, consisting chiefly of
neutrophils, in the peribronchiolar alveoli.
•ii) Thickening of the alveolar septa by congested
capillaries and leucocytic infiltration.
•iii) Less involved alveoli contain oedema fluid
34.
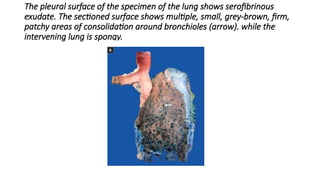
The pleural surfaceof the specimen of the lung shows serofibrinous
exudate. The sectioned surface shows multiple, small, grey-brown, firm,
patchy areas of consolidation around bronchioles (arrow). while the
intervening lung is spongy.
35.
Microscopic appearance ofbronchopneumonia. The
bronchioles as well as the adjacent alveoli are filled with
exudate consisting chiefly of neutrophils. The alveolar septa are
thickened due to congested capillaries and neutrophilic
infiltrate
36.
COMPLICATIONS.
•The complications oflobar pneumonia may occur in
bronchopneumonia as well.
•However, complete resolution of bronchopneumonia
is uncommon.
•There is generally some degree of destruction of the
bronchioles resulting in foci of bronchiolar fibrosis
that may eventually cause bronchiectasis.
37.
CLINICAL FEATURES
• Thepatients of bronchopneumonia are generally infants or
elderly individuals.
• There may be history of preceding bed-ridden illness, chronic
debility, aspiration of gastric contents or upper respiratory
infection.
• For initial 2 to 3 days, there are features of acute bronchitis but
subsequently signs and symptoms similar to those of lobar
pneumonia appear.
• Blood examination usually shows a neutrophilic leucocytosis.
• Chest radiograph shows mottled, focal opacities in both the lungs,
chiefly in the lower zones.
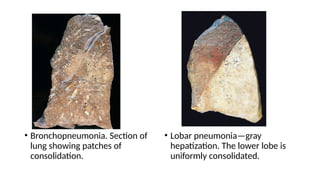
• Bronchopneumonia. Sectionof
lung showing patches of
consolidation.
• Lobar pneumonia—gray
hepatization. The lower lobe is
uniformly consolidated.
41.
VIRAL AND MYCOPLASMALPNEUMONIA
(PRIMARY ATYPICAL PNEUMONIA)
• Viral and mycoplasmal pneumonia is characterised by patchy inflammatory
changes, largely confined to interstitial tissue of the lungs, without any
alveolar exudate.
• Other terms used for these respiratory tract infections are interstitial
pneumonitis, reflecting the interstitial location of the inflammation, and
primary atypical pneumonia, atypicality being the absence of alveolar
exudate commonly present in other pneumonias.
• Interstitial pneumonitis may occur in all ages.
• Most of the cases are mild and transient; exceptionally it may be severe and
fulminant.
42.
•Etiology. Interstitial pneumonitisis caused by a wide
variety of agents, the most common being
respiratory syncytial virus (RSV).
•Others are Mycoplasma pneumoniae and many
viruses such as influenza and parainfluenza viruses,
adenoviruses, rhinoviruses, coxsackieviruses and
cytomegaloviruses (CMV).
•Occasionally, psittacosis (Chlamydia) and Q fever
(Coxiella) are associated with interstitial pneumonitis.
43.
OTHER TYPES OFPNEUMONIAS
•Some other types of pneumonias caused by
infective agents (such as Pneumocystis carinii
pneumonia and Legionella pneumonia) and
certain non-infective varieties (e.g. aspiration
pneumonia, hypostatic pneumonia)
44.
REFERENCES
1. Muir’s Textbookof Pathology, edition above 13th
2. General Pathology by Walter and Isreal
3. Robbins and Cotran, Pathologic Basis of disease,
editions above 7th
45.
ASSIGNMENT- 6.5 Inflammation(6.21, 6.22,
6.23)
• Figure 6.21- refer to Robins and Cotran page 705 fig 15.35 A
• PLEASE HAND IN ON FRIDAY MORNING(BY 9AM)







![Pulmonary_inections[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pulmonaryinections1-230718060523-80803fef-thumbnail.jpg?width=640&height=640&fit=bounds)








































![ANTIPROTOZAL_DRUGS, overview of different protozoal infections[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/antiprotozaldrugs-11-250313192836-f3e3bdb1-thumbnail.jpg?width=640&height=640&fit=bounds)





















