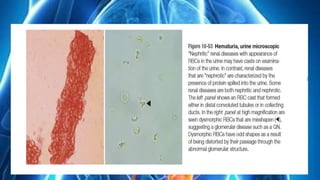
The document provides an overview of kidney tumors, categorizing them into benign and malignant types, with renal cell carcinoma (RCC) and transitional cell carcinoma (TCC) being the most common malignant forms. It outlines the signs and symptoms associated with kidney cancer, its pathophysiology, and risk factors, including age and environmental exposures. Additionally, it describes the classification and genetics of renal cell carcinomas, emphasizing the prevalence of sporadic cases linked to mutations in the VHL tumor suppressor gene.