Downloaded 616 times


























![Outpatients Treatment(empirical)
Previously healthy and no antibiotics in past 3 months:
o A macrolide (clarithromycin or azithromycin or
Doxycycline )
Comorbidities or antibiotics in past 3 months:
o Respiratory fluoroquinolone [moxifloxacin ,levofloxacin
] or β-lactam ( high-dose amoxicillin or
amoxicillin/clavulanate)](https://image.slidesharecdn.com/pneumonia-180227170058/85/Pneumonia-32-320.jpg)
![Inpatients, non-ICU
A respiratory fluoroquinolone [moxifloxacin
,levofloxacin ]
β -lactam [cefotaxime ,ceftriaxone ,ampicillin]
PLUS a macrolide [oral clarithromycin or
azithromycin)](https://image.slidesharecdn.com/pneumonia-180227170058/85/Pneumonia-33-320.jpg)
![Pseudomonas
An antipneumococcal, antipseudomonal β-lactam
[piperacillin/tazobactam, cefepime , imipenem ,
meropenem] PLUS Flouroquinolons
Above β-lactams PLUS an aminoglycoside and
azithromycin
Above β-lactams PLUS an Aminoglycoside
PLUS an antipneumococcal Fluoroquinolone](https://image.slidesharecdn.com/pneumonia-180227170058/85/Pneumonia-35-320.jpg)







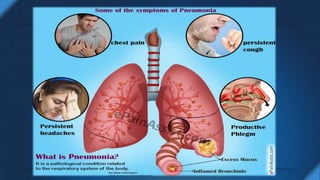
Pneumonia is an infection of the lungs that can be caused by bacteria, viruses, or fungi. It causes inflammation in the air sacs of the lungs called alveoli. Risk factors include smoking, respiratory infections, old age, and reduced immune defenses. Pneumonia is diagnosed based on symptoms, physical exam findings, chest x-ray results, and lab tests. Treatment depends on severity and may involve antibiotics, with choices guided by patient risk factors and location of care. Complications can include sepsis, lung abscess, respiratory failure, and death, especially in severe cases requiring intensive care.























































































