Downloaded 1,976 times





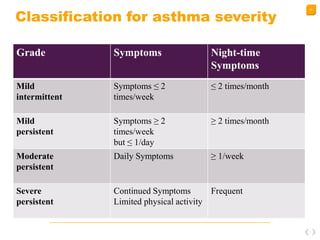








This document provides an overview of bronchial asthma, including its classification, pathophysiology, risk factors, diagnosis, and treatment. It begins with an introduction defining asthma as a chronic inflammatory airway disease characterized by wheezing and reversible airway obstruction. It then covers asthma's classification into allergic and non-allergic types, risk factors like genetics and environment, and diagnostic tests like spirometry and allergy testing. The bulk of the document focuses on treatment approaches, including non-pharmacological methods and a wide range of pharmacological options targeting inflammation and bronchodilation. It concludes with guidance on managing severe exacerbations and the goals of prophylaxis.