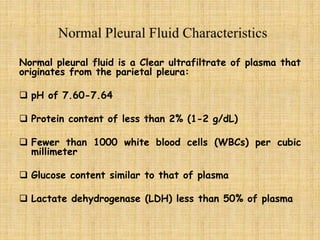
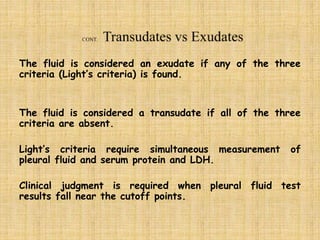
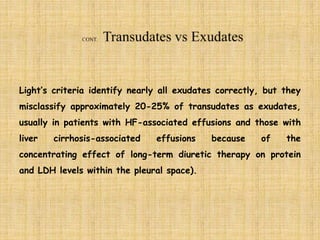
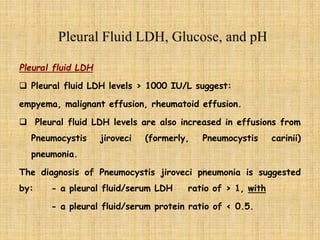
Thoracentesis should be conducted for new and unexplained pleural effusions, with the fluid characteristics indicating possible conditions such as empyema or hemothorax. Light's criteria help differentiate between exudative and transudative effusions, though misclassification can occur in certain conditions, necessitating additional tests like serum-effusion gradients. Factors like pleural fluid glucose, pH, and cytology are vital in diagnosing conditions like tuberculosis and malignancies.



![In a more recent systematic review,
• pleural fluid cholesterol greater than 55 mg/dL and
• pleural fluid LDH greater than 200 U/L
each had better positive and negative likelihood ratio for
distinguishing exudates from transudates than did Light’s
criteria. [4]](https://image.slidesharecdn.com/pleuraleffusion-final-200307045959/85/Pleural-Fluid-Analysis-11-320.jpg)















![1. https://emedicine.medscape.com/article/299959-workup
2. https://www.pulmonologyadvisor.com/home/decision-support-
in-medicine/pulmonary-medicine/hemorrhagic-pleural-
effusions-and-hemothorax/
3. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4753987/
4. Wilcox ME, Chong CA, Stanbrook MB, Tricco AC, Wong C,
Straus SE. Does this patient have an exudative pleural
effusion? The Rational Clinical Examination systematic
review. JAMA. 2014 Jun 18. 311(23):2422-31. [Medline].
5. https://www.ncbi.nlm.nih.gov/pubmed/22372660](https://image.slidesharecdn.com/pleuraleffusion-final-200307045959/85/Pleural-Fluid-Analysis-33-320.jpg)




































































