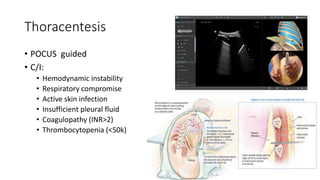
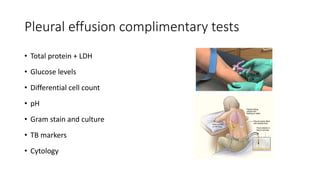
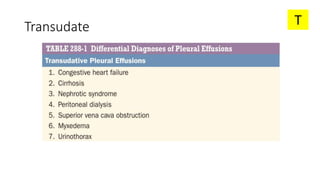
The document discusses pleural effusion, detailing its definition, signs and symptoms, diagnosis methods, and the differentiation between transudate and exudate types. It highlights common etiologies, diagnostic algorithms, and specific conditions associated with pleural effusions, such as heart failure, malignancies, and pneumonia. Additionally, it outlines the diagnostic criteria and tests necessary to determine the underlying causes and appropriate treatments for pleural effusions.