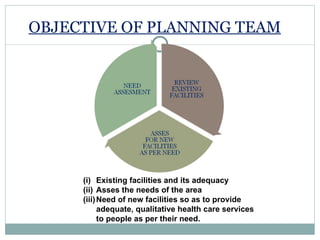
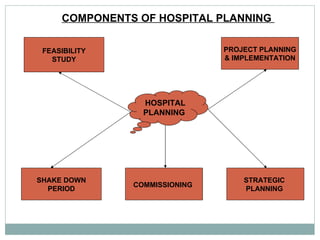
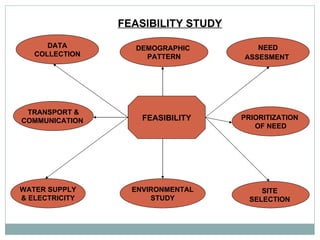
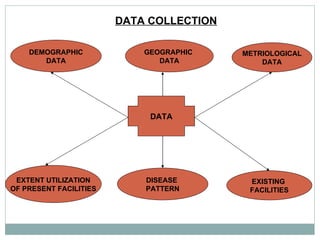
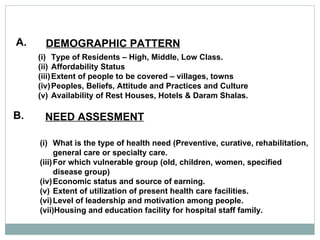
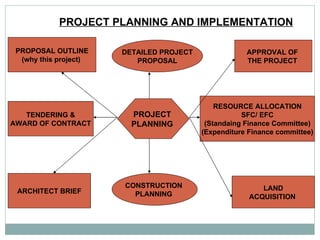


The document outlines the process for planning a new hospital, including forming a planning team, conducting feasibility studies, and implementing the project. Key steps involve assessing community health needs, selecting an appropriate site, developing construction plans, procuring equipment and staff, and commissioning the new facility once built. The planning process aims to establish adequate healthcare services through strategic planning and consideration of factors like infrastructure, resources, and community demographics.
































![Hospital licensing process_up_cph[1]](https://cdn.slidesharecdn.com/ss_thumbnails/hospitallicensingprocessupcph1-120603011737-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

















![Set Up Of New Hospital [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/setupofnewhospitalautosaved-230122155948-faa3454b-thumbnail.jpg?width=640&height=640&fit=bounds)
























































