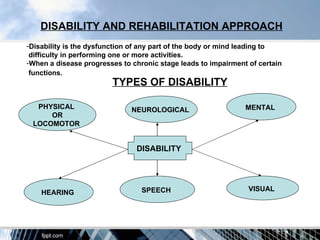
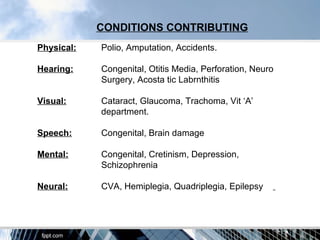
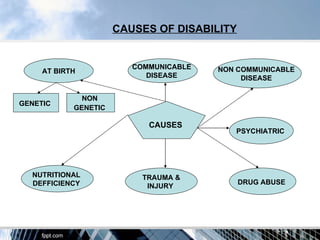
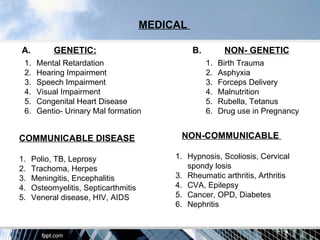
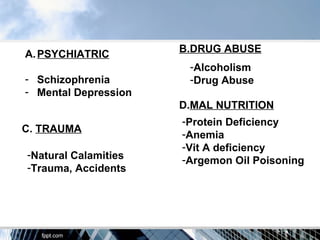
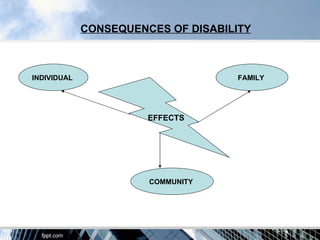


The document discusses the various aspects of disability and rehabilitation, focusing on the types of disabilities and their causes, which include communicable and non-communicable diseases, genetic factors, and trauma. It emphasizes the importance of prevention through primary, secondary, and tertiary measures, as well as the various intervention strategies—physical, psychological, educational, and vocational—that are essential for effective rehabilitation. The overall goal is to restore individuals' physical, social, and psychological potential to enable them to lead independent lives.