
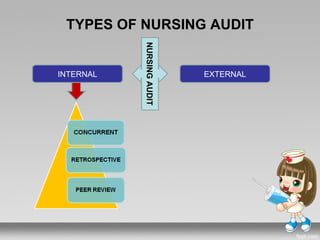
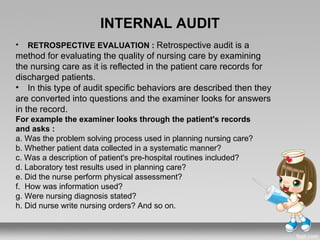
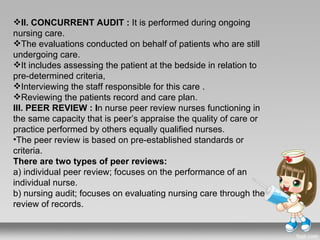
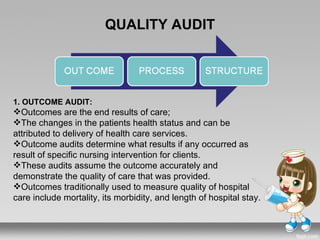
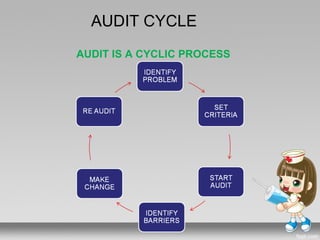
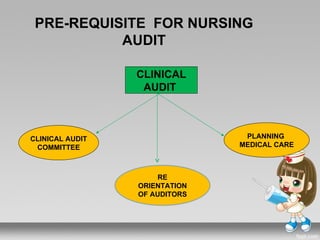


The document discusses nursing audits as a crucial mechanism for ensuring quality nursing care, detailing their history, purposes, types, and methodologies. It highlights the evolution from early clinical audits by figures like Florence Nightingale to contemporary nursing audit practices, emphasizing evaluation methods such as internal, external, retrospective, concurrent, and peer reviews. Overall, it underscores the importance of structured processes and criteria in conducting effective audits to improve nursing standards and patient care.








































































































