Downloaded 688 times
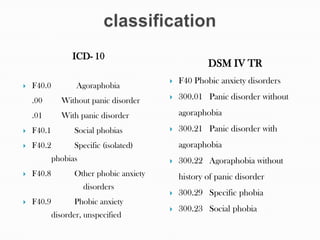



This document provides information about phobias. It defines phobias and describes their epidemiology, etiology, diagnostic criteria according to ICD-10 and DSM-IV, and treatment options including psychotherapy, behavior therapy, pharmacotherapy, and nursing management. The key points are: Phobias are irrational fears caused by classical conditioning or genetic factors. They involve disproportionate fear and avoidance of specific stimuli. Social phobia is the most common phobia. Treatment involves exposure therapy, skills training, medication, and helping patients cope with fears and social isolation. Nurses assess phobias and support patients by teaching coping strategies and gradually exposing them to feared stimuli.


























































