Downloaded 90 times
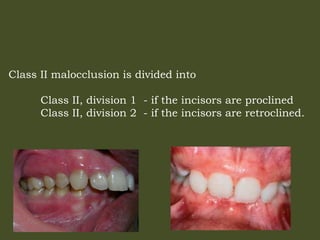






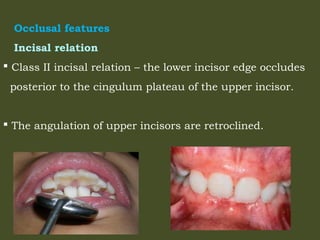
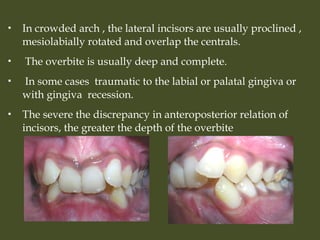
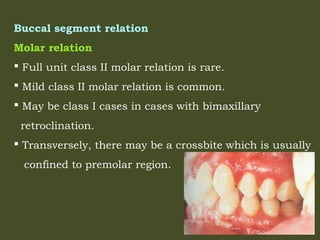
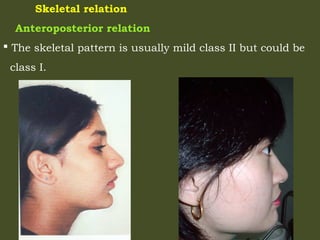

Class II malocclusions include anomalies where the mesiobuccal cusp of the maxillary first permanent molar occludes mesial to the lower first permanent molar, with variations including Class II Division 1 and Division 2 based on incisor inclination. Class II Division 1 is characterized by proclined upper incisors, prominent overjet, and potential dental anomalies, while Class II Division 2 features retroclined upper incisors, deep overbite, and possible crossbites. Both divisions exhibit distinct skeletal relations, facial growth patterns, and mandibular positioning affecting treatment approaches in orthodontics.























































































