Downloaded 43 times

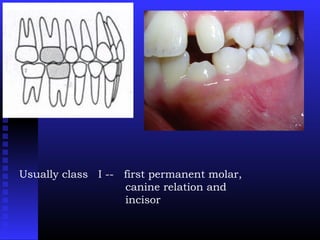





The document discusses the clinical features of malocclusion, particularly focusing on Angle's classification, which includes normal occlusion, Class I, II, and III malocclusions. Class I malocclusions generally have normal anteroposterior relationships but may show transverse or vertical discrepancies, with complications like crowding or spacing. The skeletal and facial growth patterns are typically stable, but issues can arise from dentoalveolar adaptations and soft tissue characteristics.























































































