Penetrating neck injuries can involve important structures and require careful assessment and management. The document outlines:
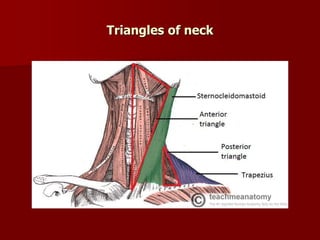
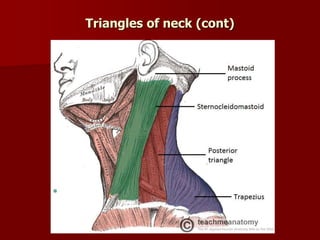
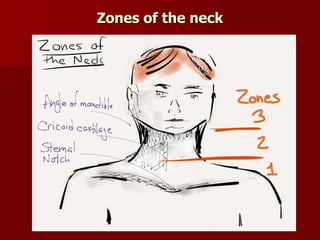
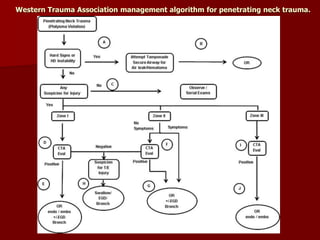
1) A classification system for penetrating neck injuries based on location and depth. Zone I injuries below the cricoid cartilage pose the highest risk to major blood vessels.
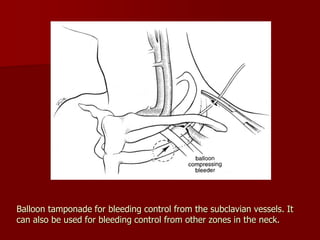
2) A primary survey approach following ATLS guidelines is recommended to assess the airway, breathing, circulation, disability and environment. Hard signs of injury to airways or blood vessels require prompt surgical management.
3) Investigation may involve imaging like CT, Doppler ultrasound or angiography to identify injuries requiring surgery versus conservative management for stable patients with no signs of major injury. Early identification of injuries allows for proper treatment to prevent complications.








![Penetrating neck trauma [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/penetratingnecktraumaautosaved-191124155903-thumbnail.jpg?width=640&height=640&fit=bounds)

















































































