













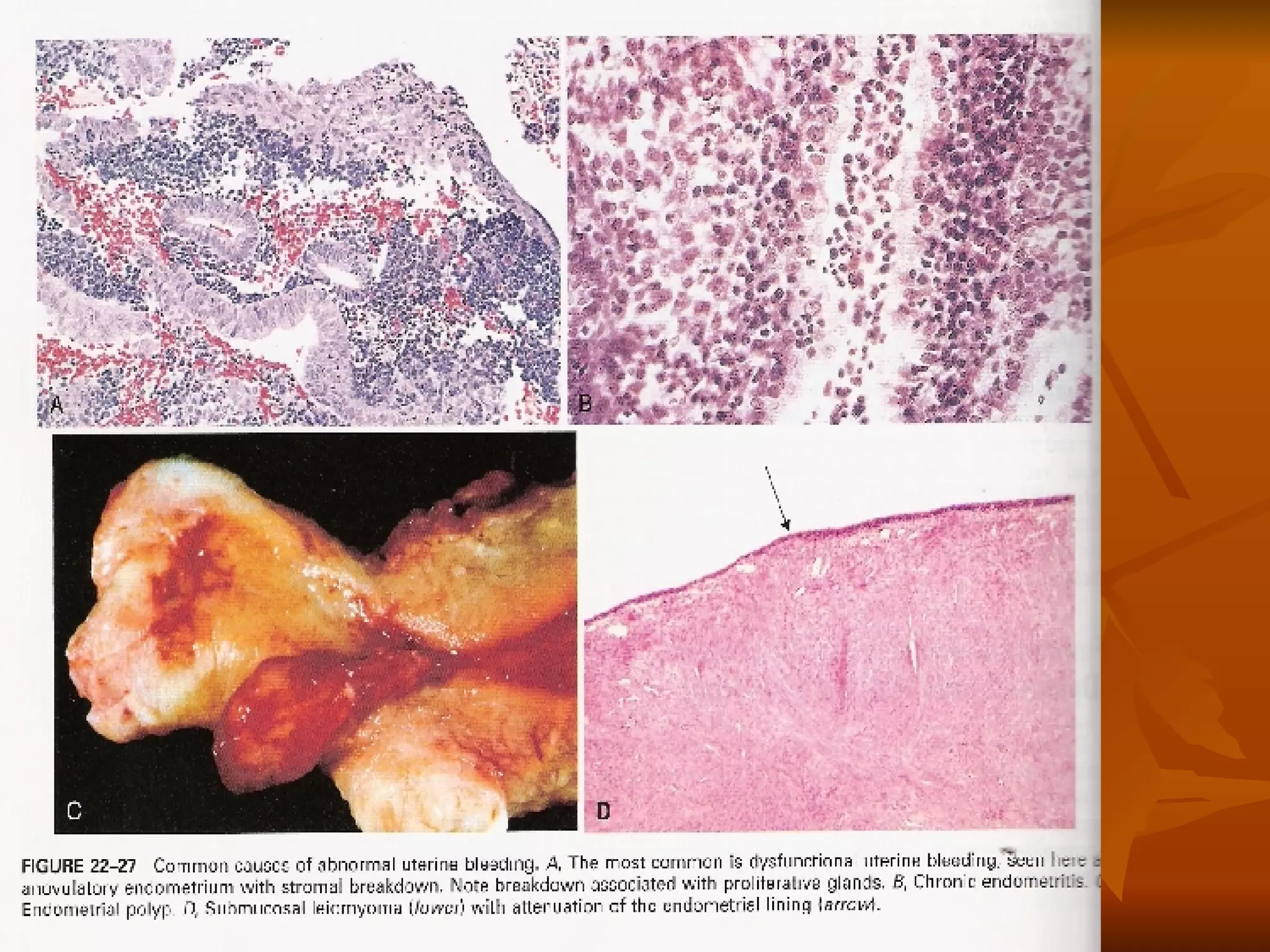



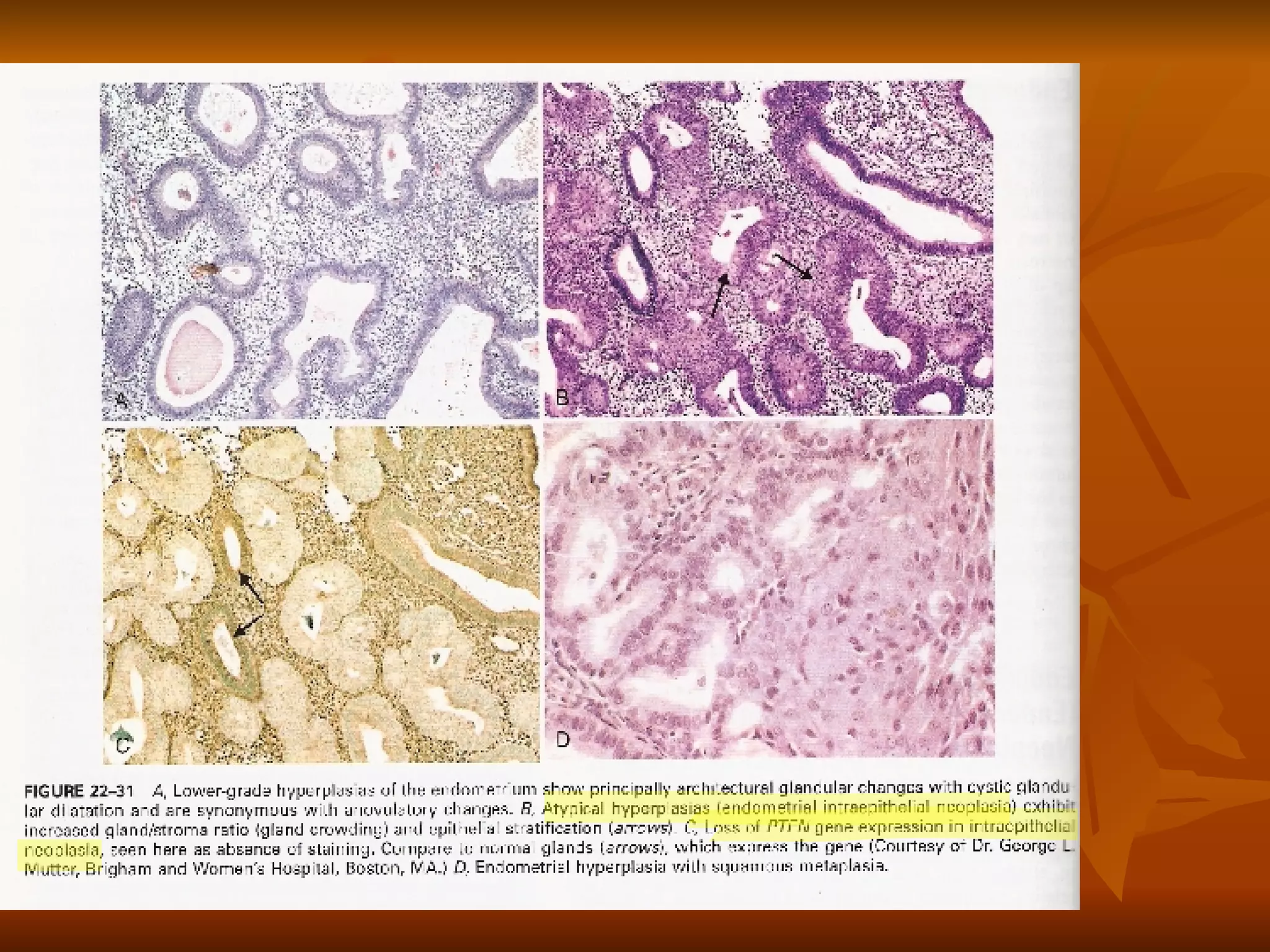


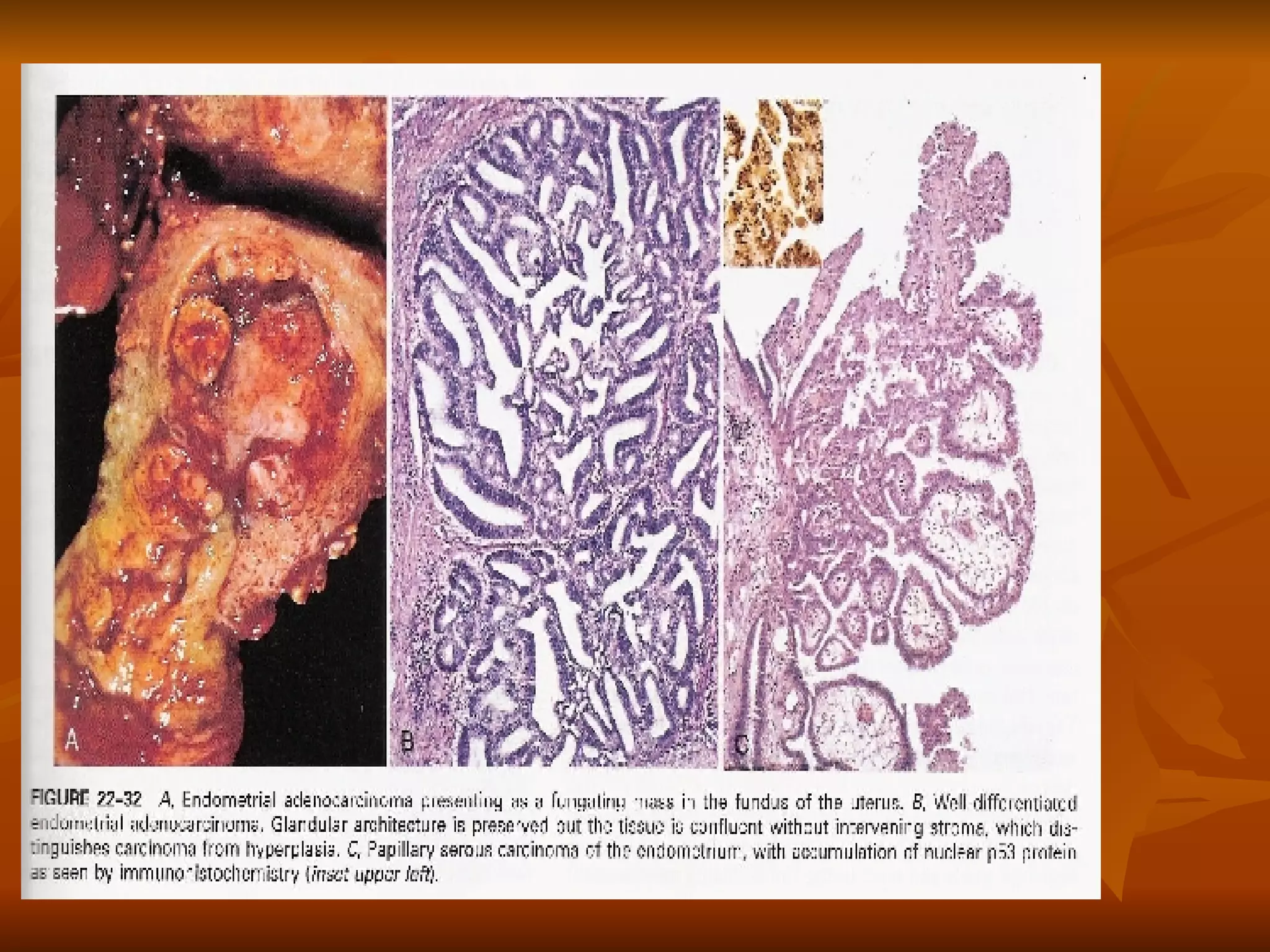
































The female genital tract is susceptible to several cancers and dysfunctions. Cervical cancer is diagnosed through cytologic screening and treated with surgical removal or vaccines. Dysfunctional uterine bleeding can result from anovulatory or inadequate luteal cycles. Endometrial cancer risk increases with age, obesity, diabetes, and nulliparity. The most common type is endometrioid adenocarcinoma. Ovarian cancer risk is higher with nulliparity, family history, and certain genetic mutations. Choriocarcinoma is an invasive cancer preceded by conditions like hydatidiform mole.