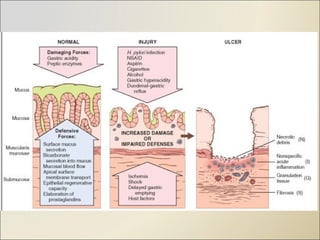
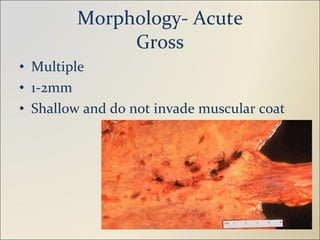
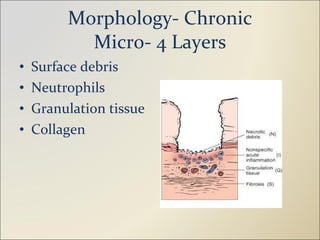
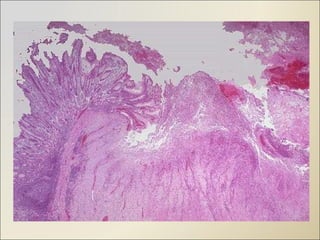
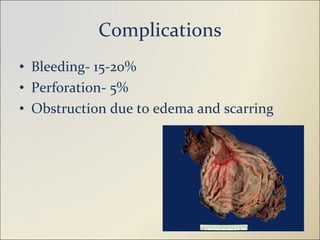
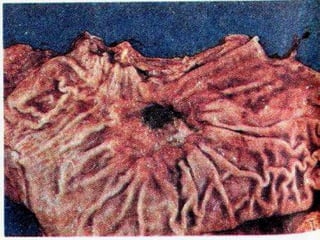
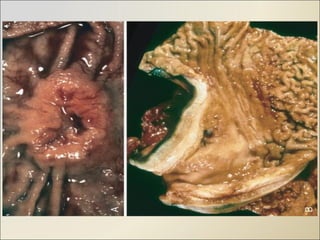
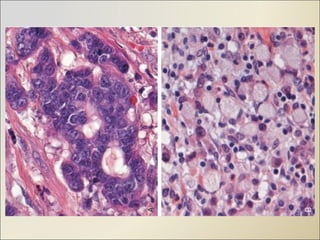
The document discusses peptic ulcers and gastric tumors. It defines a peptic ulcer and describes the etiology as being related to Helicobacter pylori infection and NSAID use. It discusses the sites of peptic ulcers as the duodenum and stomach. It also summarizes the gross and microscopic morphology of acute and chronic gastric ulcers. For gastric tumors, it classifies the main types and discusses the epidemiology, etiology, morphology, clinical features, investigations, staging, and prognostic markers for gastric carcinoma.









































![Pud Gastritis Lecture[1]](https://cdn.slidesharecdn.com/ss_thumbnails/pudgastritislecture1-1232045267191333-1-thumbnail.jpg?width=640&height=640&fit=bounds)









![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

















