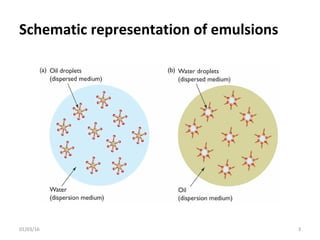
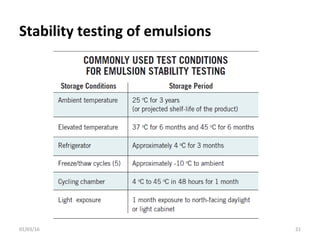
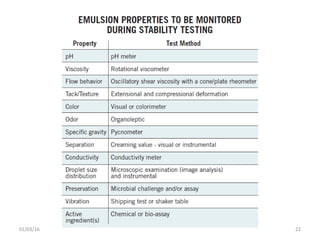
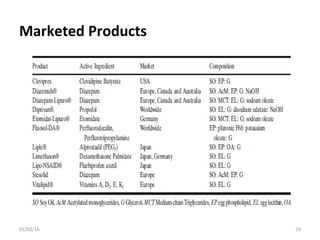
This document discusses parenteral emulsions. It begins by defining emulsions as dispersions of one liquid into another immiscible liquid, with one phase being water and the other oil. Parenteral emulsions are o/w emulsions designed for intravenous administration, with droplet sizes between 0.1-5 μm. They are used to deliver lipophilic drugs and nutrients. The document discusses the components, manufacturing, characterization, stability testing, packaging and marketed examples of parenteral emulsions. It also outlines important considerations for developing parenteral emulsions.



































![02_IJPBA_1708_18[Research]_RA.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/02ijpba170818researchra-220630064559-ddd3a137-thumbnail.jpg?width=640&height=640&fit=bounds)





































