


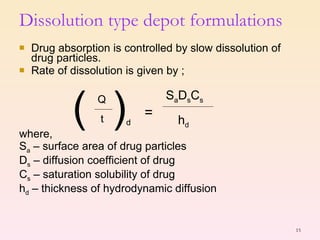
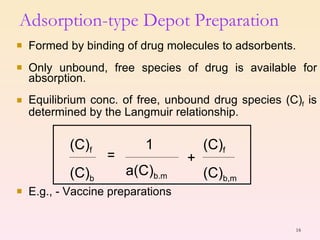
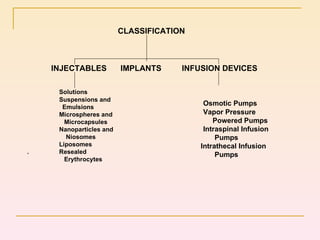

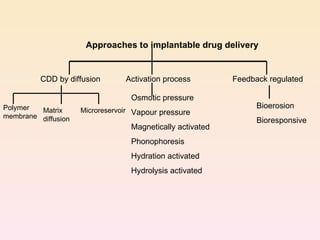




This document provides an overview of parenteral controlled drug delivery systems, including their objectives, advantages, types of formulations, approaches for formulation, routes of administration, additives used, and recent developments. The key types of formulations discussed are dissolution-controlled depots, adsorption-type depots, encapsulation-type depots, and esterification-type depots. Various approaches for implants and infusion devices are also summarized.















































































