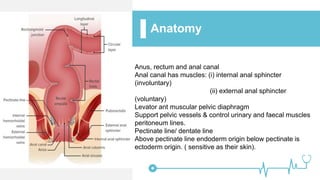
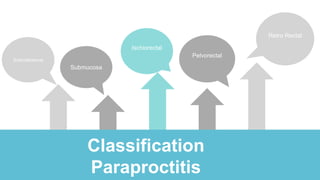
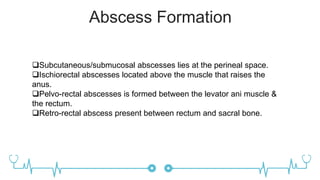
Paraproctitis is an inflammation of the tissues around the rectum and anus caused by bacteria such as E. coli and Staphylococcus aureus, resulting in a pus collection in the anorectal area. It can be classified as subcutaneous, submucosal, ischiorectal, pelvorectal, or retrorectal depending on the location of the abscess formation. Surgical drainage of the abscess is often indicated and involves making a semilunar incision to drain the pus and eliminate the internal opening using instruments such as a scalpel, clamp, and grooved probe. Complications can include spreading of the inflammation, rupture of the abscess, or burst of