The document discusses various types of pancreatic tumors including benign and malignant exocrine tumors as well as endocrine tumors. It provides details on:
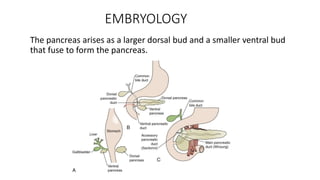
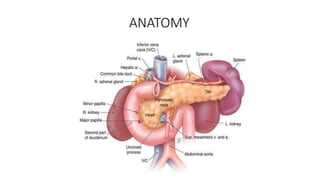
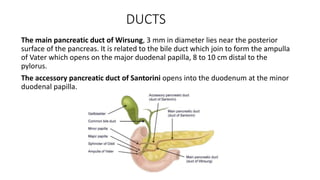
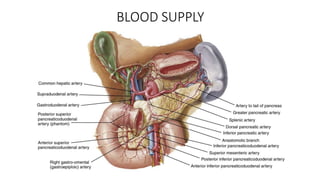
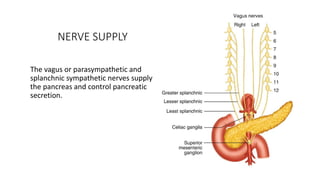
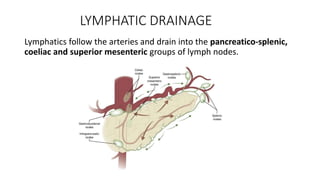
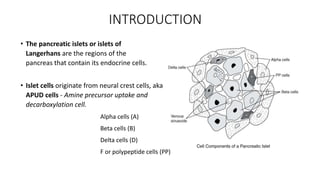
- The embryology, anatomy, blood supply, nerve supply and functions of the pancreas.
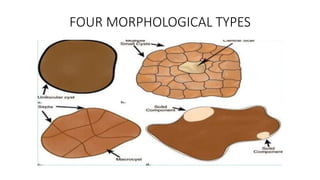
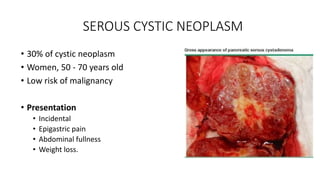
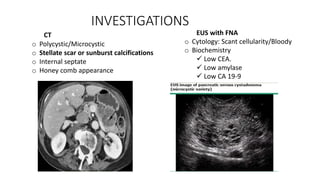
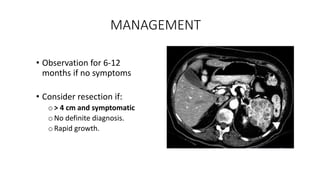
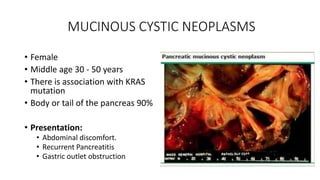
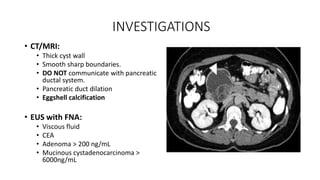
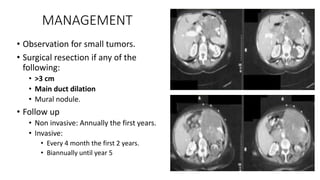
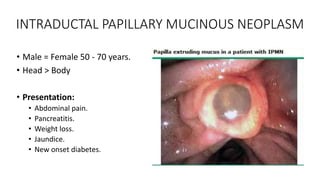
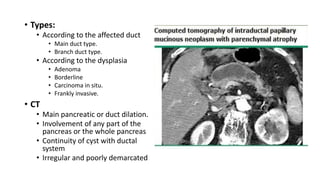
- Classification systems for benign exocrine tumors such as serous cystic neoplasms, mucinous cystic neoplasms, and intraductal papillary mucinous neoplasms.
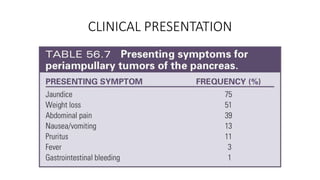
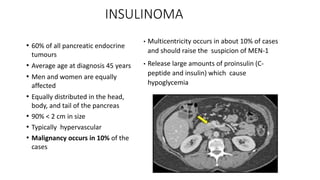
- Signs, investigations and management of insulinomas, which are the most common pancreatic endocrine tumors causing hypoglycemia.