
Recommended
More Related Content
Similar to peri ampullary carcinoma basic knowledges.pptx
Similar to peri ampullary carcinoma basic knowledges.pptx (20)
More from RupakGhimire7
Recently uploaded
Recently uploaded (20)
peri ampullary carcinoma basic knowledges.pptx
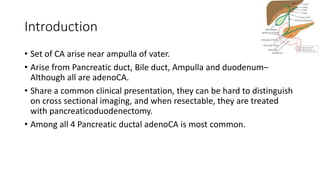
- 1. Introduction • Set of CA arise near ampulla of vater. • Arise from Pancreatic duct, Bile duct, Ampulla and duodenum– Although all are adenoCA. • Share a common clinical presentation, they can be hard to distinguish on cross sectional imaging, and when resectable, they are treated with pancreaticoduodenectomy. • Among all 4 Pancreatic ductal adenoCA is most common.
- 2. • In addition to these 4 types of adenocarcinomas, other less common tumors arise in the periampullary region including neuroendocrine tumors, acinar cell cancers, squamous cell carcinomas, gastrointestinal tumors, lymphoma, and metastases from other sites.
- 4. Pancreatic Ductal Adenocarcinoma • 3rd leading cause of CA related death in US. • In 70’s with M>F. • Risk factors includes African-American, smoking, alcohol, obesity, diabetes. • 10% are genetic- BRCA2 (familial breast and ovarian cancer), PRSS1 (hereditary pancreatitis), p16 (familial atypical multiple mole and melanoma), and HNPCC (hereditary nonpolyposis colorectal cancer).
- 5. Distal Bile Duct Cancer (Cholangiocarcinoma) • 2nd M/C peri-ampullary CA. • 30% of all CholangioCA. • In 70’s. • Risk factors for the development of cholangiocarcinoma include sclerosing cholangitis, choledochal cysts, hepatolithiasis, and infestation with liver flukes. • The common etiologic factor with these conditions is continued long- term chronic inflammation.
- 6. Adenocarcinoma of the Ampulla of Vater • 3rd in frequency. • Cause Obstructive jaundice early, hence detected early. • Biologically less aggressive. • Pancreatic, Biliary, Intestinal and Gastric type Histologically. • Intestinal type being favourable prognosis.
- 7. Duodenal Adenocarcinoma • Least common, M=F, 70’s • Develop in background of polyps like colonic CA. • In case of multiple polyps- FAP should be ruled out. • Presents with GOO, SOJ depends on location. • Usually present late. • Better stage by stage prognosis as compared to Pancreatic and CholangioCA counterpart.
- 8. Clinical Presentations • Delay diagnosis, 80% presents in Metastatic or unresectable stage. • The combination of jaundice (painless or painful) with pruritus, acholic stools, and tea-colored urine in the absence of acute biliary disease is a constellation of symptoms that should prompt the suspicion of a periampullary tumor. • Other relatively nonspecific symptoms such as Unintended wt loss, malaise, fatigue, anorexia, indigestion, or early satiety are often noted upon evaluation.
- 9. • Signs of pancreatic insufficiency (malabsorption, frequent fatty or floating stool) would suggest obstruction of the main pancreatic duct, whereas nausea and vomiting would suggest gastric outlet or duodenal obstruction. • A quite subtle sign, but one that is now known to be associated with the ultimate diagnosis of pancreatic malignancies, is the rather sudden development of adult-onset diabetes in previously healthy patients in their sixth decade of life.
- 10. • Physical exam findings include scleral icterus, jaundice, and skin excoriation from pruritus and scratching. • The Courvoisier sign, noted by palpation of an enlarged gallbladder, may be present without peritoneal signs. • More advanced disease may include the findings of cachexia, palpable left supraclavicular lymph nodes (Virchow node), palpable periumbilical nodes (Sister Mary Joseph node), and palpable pelvic metastatic disease on a rectal exam (Blumer shelf).
- 11. Labs • CBC/KFT/LFT/PT-INR. • Conjugated Hyperbilirubinemia with elevated Alkaline Phosphatase. • CA 19-9 with caution.
- 12. Imaging Evaluation • A dedicated, fine-cut, 3phase pancreas protocol computed tomography (CT) scan provides valuable information regarding local (primarily vascular) and regional (primarily the liver as the most common site of metastasis) spread of disease. • In patients with CT contrast allergy- MRI with MRCP can be done. • Cross sectional imaging is important for Extent, Stage and Potential resectability of disease.
- 14. • After ruling out metastasis, relation with nearby structures should be established– IVC, PV, SMA, SMV, CT, HA. • Abutment or involvement of above mentioned structures changes management planning. • More detail examination for relationship assessment can be done using EUS. • Possible FNA is a advantage often not required in every case except for Neo-adjuvant, palliative care. • PET-CT often used in combination but only role is to rule out metastasis.
- 15. 15
- 16. Biliary Decompression and Tissue Diagnosis • ERC is another modality of use in setting of Jaundiced patient. • Although not required in all cases where diagnosis in fairly obvious, but can be used for supporting diagnosis and Brush cytology. • Main findings on ERC includes- Abrupt cut off and Double duct sign. • Other role is in stenting in setting of Periampullary CA. • Main indications--- Before Cholangitis, Significant nutritional deficiency, Neo-adjuvant, Palliative care. • In resectable tumor- No role in jaundice between 2.3-14.6%, but can be justified if surgery is delayed >7 days.
- 18. Neoadjuvant Therapy Arguments used for administration of neoadjuvant therapy include the following: • High risk of undiagnosed stage IV disease (15%-30%); • Conversion of locally unresectable disease to resectable disease (15%-40%); • Preoperative radiation given in well-vascularized tissue may be more effective; • Preoperative selection tool in patients with marginal candidacy for surgery from a general medical standpoint; • Increase in margin-negative resection rate; • and most patients will receive some form of chemotherapy or radiation (up to 100%), as opposed to the large number of patients having to omit or delay adjuvant therapy secondary to postoperative complications (up to 40%).
- 19. • Although NA CRT is most studied in resectable disease, but have no well defined role in this setting. • Defined role in Borderline resectable disease and unresectable disease.
- 20. Borderline resectable The Americas Hepatopancreatobiliary Association/Society for Surgery of the Alimentary Tract/Society of Surgical Oncology/National Comprehensive Cancer Network definition of borderline resectable pancreatic tumors includes the following: (1) venous involvement of the SMV/PV demonstrating tumor abutment, encasement, short segment venous occlusion but with suitable vessel proximal and distal to the area of the vessel involvement, for safe resection and reconstruction; (2) gastroduodenal artery encasement up to the hepatic artery and short segment encasement/direct tumor abutment of the hepatic artery with no extension to the celiac trunk; and (3) less than 180degree involvement of the SMA. A more recent simplified definition by Cao et al used a tumor vein circumferential interface grouping (TVI) system, as follows: no interface, <180 degrees of vessel circumference, or >180 degree of vessel circumference or occlusion.
- 21. Common practice • FOLFIRINOX, nab-paclitaxel, and gemcitabine based therapy is most commonly used. • Starts with Induction CT, with radiation of 50.4Gy in 1.8#. • Evaluation afterward and if feasible surgery within 4-8weeks.
- 22. SURGICAL APPROACHES • Diagnostic laparoscopy depending on institution protocol--- Advised for bulky mass, CA body and tail, CA19-9 >200U/L. • Exploration--- Assessment--- Resection--- Reconstruction.
- 23. Whipple’s Procedure • Allen Oldfather Whipple; Kausch-Whipple • Removal of HOP, Duodenum, part of Jejunum, Gall bladder, Distal Stomach, Bile duct • Reconstruction – PJ, HJ, GJ, + FJ • 5-6 Hrs; 2% Mortality; 40% complications 23
- 24. 24
- 25. 25
- 26. 26
- 27. 27
- 28. Variations • Pylorus preserving • Pancreato-gastrostomy instead of PJ 28
- 29. 16 studies 1629 patients No difference in POPF Rates Perivoliotis K et al. Int J Surg Oncol. 2017;2017:7526494
- 30. Palliative Operations • End to side HJ. • Gastro-Jejunostomy. • Pain palliation--- Chemical/Surgical Splanchinectomy.
- 31. Some controversies • Classical vs PPPD. • SMA 1st. • PJ vs PG. • Lymphadenectomy. • Associated liver resection. • Splenectomy. • Open vs Lap vs Robotics. • Drain vs No drains.
- 32. Post op Complications • Low rates in High volume centres--- 10-12 cases/year. • Although postsurgical mortality in high-volume centers is low (0%- 3%), postoperative morbidity continues to remain high (30%-50%). • The frequent serious postoperative complications are delayed gastric emptying (15%-20%), pancreatic anastomotic leak (10%-20%), wound infection (8%-10%), intra-abdominal (8%-10%) abscess, postoperative hemorrhage (1%-8%), and pancreas fistula (5%).
- 33. The International Study Group of Pancreatic Surgery • Post pancreatectomy hemorrhage has been categorized by 3 important parameters: onset (before or after 24 hours from the time of surgery), location (intra- or extraluminal), and severity (low or high). • Delayed gastric emptying has been defined as the inability to return to a standard diet by the end of the first postoperative week. Categories of A, B, and C have been established considering the inability to tolerate solid food by 7, 14, or 21 days or nasogastric tube requirement by 3, 7, or 14 days postoperatively or reinsertion of a nasogastric tube between the days mentioned above.
- 34. • Postoperative pancreatic fistula has been defined as drain output of any measurable volume of fluid on or after POD 3 with amylase content greater than 3 times the serum amylase activity, with the following grades established: A (no clinical impact), B (deviation from normal postoperative course, percutaneous drain placement), or C (reoperation or death).
- 35. Prognosis • Only 15% have curative resection. • Poor 10 year survival of 3.9%. • A recent paper using a large population-based dataset identified lymph node ratio (number of nodes harboring disease/total number of nodes examined), margin status, adjuvant chemotherapy, and pathologic T stage as being the top 4 variables associated with long- term survival in pancreatic cancer patients.
- 36. Adjuvant Therapy • Role is controversial--- Morbid surgery. • If given--- After 1-2 months--- Often delayed due to complications. • Phase 3 EORTC– RT+5FU CT vs Observation following curative intent surgery– Similar 2 year OS and PFS. • ESPAC 3- Showed no advantage of Gemcitabine over 5FU based regimen. • Although overall FOLFIRINOX is beneficial in Locally advanced setting. • ESPAC-4 brings out beneficial role of addition of Capecitabine to Gemcitabine regimen.
- 37. • Role of radiation in adjuvant setting is more controversial--- ESPAC-1 sowed detrimental effect of radiation in adjuvant setting. • ABC 02 trial showed beneficial role of Cisplatin with Gemcitabine in locally advanced and metastatic setting.
- 39. Immunotherapy • Defined role in Melanoma and RCC. • Being studied in Pancreatic adenoCA. • The purpose of immunotherapy is to activate both the cellular and humoral immune components of the immune system. • Patients with higher levels of CD4+ and CD8+ tumor-infiltrating lymphocytes had longer overall survival after surgical resection. • Since 1995, there have been 4 peptide vaccine trials, 2 recombinant vaccine trials, 1 dendritic cell vaccine, 4 whole cell vaccines, and 1 combination immunotherapy trial--- results are not encouraging.
- 40. • Peri-ampullary adenoCA are immunotolerant. • The future of pancreatic cancer immunotherapy lies in identifying more tumor antigens, targeting multiple antigens, incorporating checkpoint blockade inhibitors, and tumor microenvironment manipulation.